We use cookies to enhance your browsing experience, serve personalized ads or content, and analyze our traffic. By clicking "Accept All", you consent to our use of cookies.
Customize Consent Preferences
We use cookies to help you navigate efficiently and perform certain functions. You will find detailed information about all cookies under each consent category below.
The cookies that are categorized as "Necessary" are stored on your browser as they are essential for enabling the basic functionalities of the site. ...
Always Active
Necessary cookies are required to enable the basic features of this site, such as providing secure log-in or adjusting your consent preferences. These cookies do not store any personally identifiable data.
Cookie
cookieyes-consent
Duration
1 year
Description
CookieYes sets this cookie to remember users' consent preferences so that their preferences are respected on subsequent visits to this site. It does not collect or store any personal information about the site visitors.
Functional cookies help perform certain functionalities like sharing the content of the website on social media platforms, collecting feedback, and other third-party features.
Cookie
_dc_gtm_UA-*
Duration
Less than a minute
Description
Google Analytics sets this cookie to load the Google Analytics script tag.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics such as the number of visitors, bounce rate, traffic source, etc.
Cookie
_gcl_au
Duration
3 months
Description
Google Tag Manager sets the cookie to experiment advertisement efficiency of websites using their services.
Cookie
_ga
Duration
1 year 1 month 4 days
Description
Google Analytics sets this cookie to calculate visitor, session and campaign data and track site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognise unique visitors.
Cookie
_gid
Duration
1 day
Description
Google Analytics sets this cookie to store information on how visitors use a website while also creating an analytics report of the website's performance. Some of the collected data includes the number of visitors, their source, and the pages they visit anonymously.
Cookie
_gat_gtag_UA_*
Duration
Less than a minute
Description
Google Analytics sets this cookie to store a unique user ID.
Cookie
_ga_*
Duration
1 year 1 month 4 days
Description
Google Analytics sets this cookie to store and count page views.
Cookie
_gat_UA-*
Duration
Less than a minute
Description
Google Analytics sets this cookie for user behaviour tracking.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
No cookies to display.
Advertisement cookies are used to provide visitors with customized advertisements based on the pages you visited previously and to analyze the effectiveness of the ad campaigns.
Throughout June, thousands of supporters in nearly 50 communities gathered across the country to raise funds for type 1 diabetes (T1D) research.
Breakthrough T1D Walk (formerly the JDRF Walk to Cure Diabetes) is the largest fundraising event in Canada that unites the T1D community who are dedicated to making every day better for the estimated 300,000 Canadians living with type 1 diabetes (T1D), as we drive toward curing this disease. Breakthrough T1D Walk has raised more than $143 million to date in its over 30-year history, making it one of the longest running and most successful fundraising events in the country.
The collective fundraising goal is $3.2 million that will help support Breakthrough T1D Canada’s mission to find cures for T1D, and to date more than $2.5 M has already been raised through 1312 teams, 9112 participants and 17807 donations!
Additional Walks took place in May with several communities still planning Walks in the Fall, including schools participating as part of our Breakthrough T1D School Walk Program, where schools across the country can host Walks supported by their students and teachers throughout the year.
This year has truly been a national effort with Walks taking place in every province, from Newfoundland to Vancouver Island, and even with Walk Your Way events happening in Yukon and Nunavut.
The Walk is so much more than just a fundraiser. It’s a chance for families living with T1D to meet, share their stories, and gain support from each other. Many Walks had a tent for newly-diagnosed families, manned by volunteers who have lived through a T1D diagnosis and were available to offer support, resources, and encouragement.
There were exciting kids’ games, activities from our corporate sponsors, Star Wars characters, amazing custom-made Team t-shirts, face-painting, and so much more! Each Walk location had their own unique offerings to make the day one to remember for all the participants.
At the Breakthrough T1D Walk in Toronto, we were once again joined by Breakthrough T1D ambassador Max Domi. Max met with families, took hundreds of selfies with fans, signed countless autographs and shared a bit of his T1D story from the stage, especially noting the role his parents played (who were both in attendance) in helping him learn to manage his T1D and help smooth his path to the NHL. As always, Max was generous, welcoming and brought hope and inspiration to attendees, particularly our newly-diagnosed families.
We want to thank our Walk Ambassadors who are helping to break the stigma of living with T1D, paving the way for a new generation of younger people living with T1D who are fiercely proud and committed to making life better today while we work towards a tomorrow free from T1D. They are so inspiring, and we thank each of them for their efforts and enthusiasm.
Thank you as well to our corporate partners, whose support helps us to build a special day of community spirit, along with important resources for T1D families, particularly those new to T1D.
Thank you to our amazing and tireless Breakthrough T1D Volunteer Committees and our staff who spend months working to ensure that the Walks run smoothly and that our participants have the best possible experience.
Our Breakthrough T1D Walks simply couldn’t happen without our incredible Walkers, volunteers, donors, vendors, and our local, regional, and national partners. Truly, we can’t do it without you.
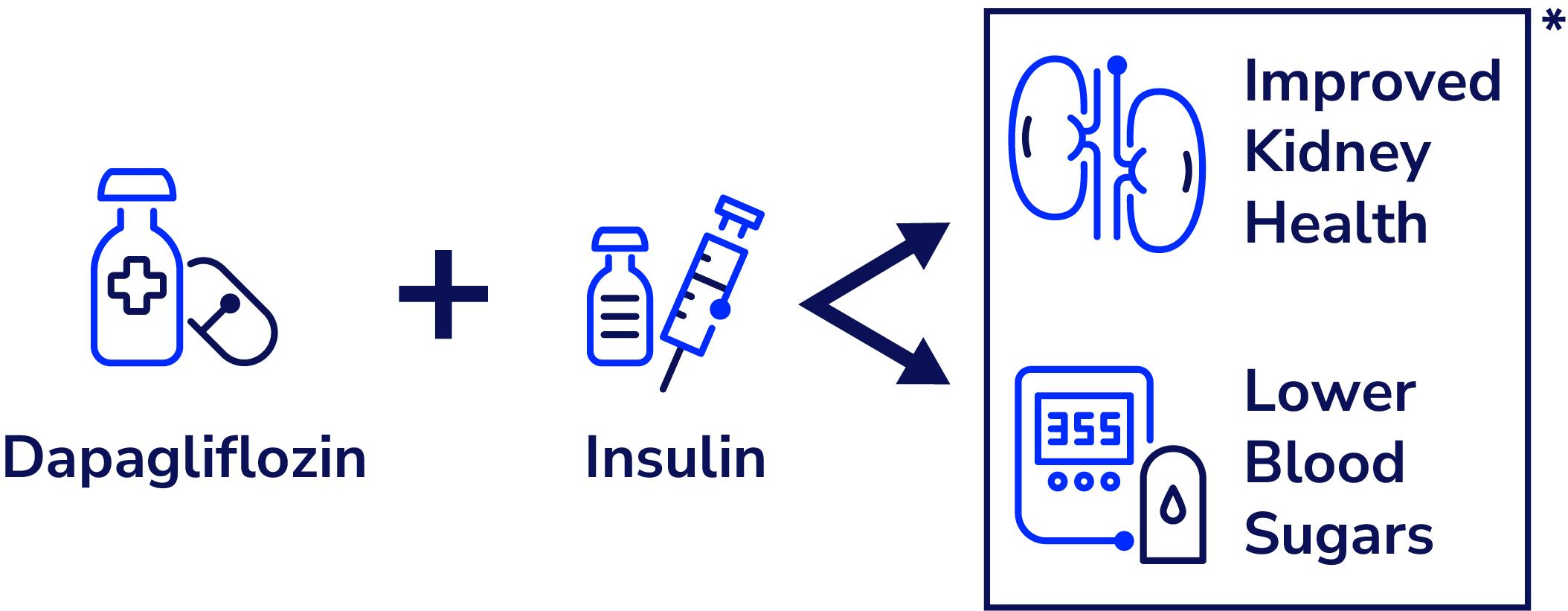
Dapagliflozin, an SGLT2i medication often used for people with type 2 diabetes, showed improved kidney function and glycemic management in teens with type 1 diabetes. This trial supports a growing body of evidence that supports the use of adjunctive therapies (drugs beyond insulin) for T1D.
Adolescence can be a challenging time to manage type 1 diabetes (T1D). Life (and hormones!) change in all sorts of ways, and many teenagers experience higher than recommended blood glucose levels as a result, which can mean an increased risk of complications later in life. The study of novel therapies that can improve glycemic control in teens with T1D and reduce the risk of diabetes complications is critical to improving the lives of youth living with diabetes.
Adjunct-to-insulin therapy – i.e., taking another drug alongside usual insulin treatment – is one approach that could help on both fronts. For example, sodium-glucose cotransporter-2 (SGLT2) inhibitors are a class of oral medications approved for type 2 diabetes that reduce glucose from the blood from being absorbed by the kidneys, instead encouraging glucose to be released in urine. Dr. Farid Mahmud and his team at the Hospital for Sick Children (SickKids) in Toronto conducted a clinical trial that tested the safety and efficacy of an SGLT2 inhibitor called dapagliflozin in teens with T1D. The ATTEMPT trial (Adolescent Type 1 Diabetes Treatment with SGLT2i for Hyperglycemia & Hyperfiltration) was funded as part of the Breakthrough T1D – CIHR Partnership to Defeat Diabetes.
The ATTEMPT study
The ATTEMPT trial aimed to determine the safety and effectiveness of an SGLT2 inhibitor called dapagliflozin on managing blood glucose and on improving kidney function in adolescents aged 12 to 18 with T1D. The study had two main goals:
To determine how effective dapagliflozin would be at improving kidney function and glycemic management; and
To determine if the drug increased the risk of diabetic ketoacidosis (DKA) and if additional safety measures could mitigate any increased risk
ATTEMPT was led by Dr. Farid Mahmud, an endocrinologist and researcher at The Hospital for Sick Children in Toronto.
A total of 98 participants and their families attended 5 in-person visits over 22 weeks and were given a random assignment to the dapagliflozin group, or the placebo group (a small pill that contains no active medicine). During the study, participants kept taking insulin, wore a continuous glucose monitor (CGM), tested for blood ketones, and were to report any adverse events. Over 850 potential participants were approached over the course of 2-years to take part in the study.
Results:
ATTEMPT is the first of its kind, landmark trial designed to evaluate the effectiveness of SGLT2 inhibitors to optimize diabetes control and prevent early subclinical kidney complications in an at-risk pediatric population with T1D.
Efficacy:
The study showed that a low dose of SGLT2 inhibitor could safely be given to youths and adolescents to improve kidney function as well as improve glycemic management. There was a clinically significant decline in HbA1c of 0.47% in the treatment group as well as a 9% increase in average time in range from CGM metrics. There was no change in the total daily insulin dose.
Safety:
The trial was designed with strict safety protocols to mitigate the risk of diabetic ketoacidosis. In collaboration with patient-partners (those living with and caregivers of individuals with T1D) a DKA Risk Mitigation Strategy was employed due to the increased risk of DKA during euglycemia (normal range glucose levels). The protocol included routine ketone monitoring with guidance for action above the threshold of 0.6 mmol/L.
Dapagliflozin was well tolerated with no study-related serious adverse events. There were no significant differences in the proportion of participants who experienced elevated ketone levels, hypoglycemia and genitourinary tract infections in the Dapagliflozin vs Placebo groups. A single case (N=1) of mild DKA was seen in the Dapagliflozin group. While rates of DKA were low, a greater number of elevated blood ketone events ≥0.6mmol/L were seen in the Dapagliflozin group (n=106) vs Placebo group (n=62) (P<0.001), demonstrating the importance of the patient-centered DKA Risk Mitigation Education strategy operationalized during the study.
The results from ATTEMPT will hopefully pave the way for further research and longer studies on the potential benefits of using adjunctive therapies to help manage type 1 diabetes.
Please note that dapagliflozin, or any SGLT2 inhibitors are not approved for individuals with T1D by Health Canada.
Mahmud, F.H., Bjornstad, P., Clarson, C. et al. Adjunct-to-insulin therapy using SGLT2 inhibitors in youth with type 1 diabetes: a randomized controlled trial. Nat Med (2025). https://doi.org/10.1038/s41591-025-03723-6
Clinical trial participation is crucial for moving forward vital T1D research from the lab to the people who need it most. To find T1D trials that are recruiting participants, and if you qualify, please visit: clinicaltrials.breakthroughT1D.ca.
On Jan 7, 2025 (Sweden), Sana Biotechnology released significant clinical data: the first person with type 1 diabetes (T1D) who received deceased donor islets engineered to evade the immune system is producing insulin without immunosuppression.
UPDATE: June 23, 2025 Sana Biotechnology presented updated data on June 23, 2025 at the six-month follow up timepoint. The single patient dosed with hypoimmune donor islets continues to produce insulin in response to a mixed meal tolerance test (MMTT) without the use of immunosuppressants.
The details
This is a big step for cell-based therapies for potentially curing T1D. Sana’s first-in-human study consists of allogeneic islets, meaning they are derived from an external source, which in this case is the pancreases of deceased donors. These islets were engineered to avoid recognition by the immune system (hypoimmune) and were implanted intramuscularly into a person with T1D. After four weeks, circulating C-peptide increased, meaning that the beta cells are alive, healthy, and producing insulin—all without the need for immunosuppression and no safety issue. This is the first evidence of engineered islets successfully avoiding immune destruction.
What this means for the T1D community
While this is an incredibly promising step forward for the T1D community, to have allogenic cells survive without the use of immunosuppressants, this trial relied on deceased donor cells, of which there will never be enough to provide to everyone living with T1D. The trial was done in a single participant and is reporting only 4-weeks of data – this is a proof-of-concept study that is promising but very preliminary.
What’s next: lots to look forward to
Breakthrough T1D believes that the best chance for T1D cures lies in stem cell-based therapies since deceased donor islets are in short supply, while stem cell-derived islets can be produced at scale. Engineering cells to evade immune attack is a new path forward to protect the insulin-producing beta cells and avoid the use of immunosuppressants. Most importantly, this technology is being studied to apply to stem cell-based therapies, which is a scalable solution for many more people with T1D. This hypoimmune technology moves us closer to the possibility of having enough immune-evading cells for everyone with T1D.
While this approach will take significant time, effort, and money, every day we take another step toward a possible life-changing T1D cure.
Breakthrough T1D’s Role
The primary objective of Breakthrough T1D’s beta cell replacement efforts is to place insulin-producing cells into people with T1D without the use of immunosuppressants. Breakthrough T1D strongly supports the development of stem cell-based therapies that do not require broad immunosuppression and Breakthrough T1D International based out of the US recently launched an initiative to accelerate this faster than ever (Project ACT – Accelerate Cell Therapies). To contribute to the advancement of these game-changing therapies, the T1D Fund: A Breakthrough T1D Venture invested in Sana recognizing that their hypoimmune engineering technology held significant promise for T1D cell therapies. We look forward to seeing how the trial progresses.
Kendra Fisher is a former member of Team Canada’s hockey program, a 3x world inline hockey champion, and a firefighter. She is also the Founder of Mentally Fit; a professional speaker, a mental health coach, and an author in the making. Kendra may be best known for her hockey career, and for making the life-altering decision to step away from her dream of playing for Team Canada in order to manage diagnoses of Generalized Anxiety Disorder, Panic Disorder, Clinical Depression, Agoraphobia, and OCD.
Kendra has been open about her journey with mental illness, and deeply vulnerable in sharing the devastating loss of her son, River, at 32 weeks gestation. When her son Bodhi was a toddler, he was diagnosed with type 1 diabetes (T1D). Now a Breakthrough T1D Canada Ambassador, Kendra is also involved with the Breakthrough T1D Walk in Toronto. She recently sat down with Breakthrough T1D Canada to share how her family navigated Bodhi’s diagnosis, all in the wake of infant loss and during the challenges of the pandemic.
Breakthrough T1D Canada: Can you share a little about the time of Bodhi’s diagnosis?
Kendra:
It was during COVID, so everything already felt intense and overwhelming. I was working as a full-time firefighter, on shift in a high-stress environment. Fortunately, Bodhi’s other mom, Kristy, was incredibly intuitive and picked up early signs that something wasn’t right.
Bodhi had been drinking constantly; he’d go from glass to glass, drinking everyone’s water. At first, we didn’t think too much of it. On its own, the thirst didn’t seem alarming. But at the same time, he was soaking through diapers. We started doubling up, laying down crib liners, trying everything, and nothing worked.
Kristy kept raising concerns that this was something more serious. Having lost our son, I was sure we were being hypervigilant—looking for problems, being too cautious. But one morning, Bodhi decided he was only going to use the potty, and by 11 a.m., he’d filled it ten times. Kristy messaged me as I was coming off shift and said she was taking him to the urgent care clinic at St. Joe’s.
Just based on those two symptoms, they checked his blood sugar, and it was incredibly high. We were told he was likely in DKA and that we either needed to admit him immediately or take him by ambulance to Sick Kids to begin treatment.
Because of COVID protocols, only one parent could go into the hospital. Kristy went in with him while I waited outside. I’ll never forget that call, Kristy was crying. She told me the doctor was coming to meet me in the lobby to give permission for me to come in. That’s where I was told, face to face, “He has diabetes.” Sick Kids would be overseeing his care.
The surreal part was that those were the only symptoms; excessive thirst and urination. He was otherwise his normal, happy, outgoing self. They got him on an IV right away and started titrating insulin. It was all happening so fast, trying to understand what was going on while still in complete shock.
They later got a more precise ketone reading and, miraculously, Bodhi wasn’t in full DKA. They called him a “warrior.” He had somehow drunk enough water to flush out the ketones. At 6 p.m. that same day, they told us we could take him home.
As a firefighter, my only experience with diabetes was responding to people in crisis. From that limited perspective, it didn’t seem possible that it was safe to bring him home. But that was day one of our new life.
And we were navigating all of this in isolation. One parent at appointments. We’d just lost River. We had our older son, Finley, who was five at the time, and the last time we had gone to the hospital for his baby brother, we came home alone. His fear was enormous. He was terrified for his little brother. As a family, we had to divide and conquer. Bodhi went straight into diabetes day care at Sick Kids the next day, and we were thrown into this world we didn’t yet understand.
Breakthrough T1D Canada: What do you want other parents to understand about type 1 diabetes?
Kendra:
I truly believe people mean well when they share their responses to learning about Bodhi; they want to help, be kind, and be supportive. But a lot of people confuse type 1 diabetes with type 2 diabetes. We were met with well-meaning, but misinformed advice. People telling us Bodhi would be fine if we cut out sugar or junk food. A friend giving him an apple instead of a lollipop, not realizing I hadn’t accounted for it in his insulin dose and that it didn’t matter that it was a healthy snack.
Others suggested things like a keto diet so he wouldn’t need insulin. And while these suggestions might come from a good place, they can be exhausting to correct, especially when you’re still trying to understand it all yourself.
Even those with experience of T1D can sometimes overwhelm you with too much information. In the beginning, it felt like there was no soft place to land. No clear starting point. This diagnosis doesn’t just affect your child; it affects your whole family.
Finley has been an incredible big brother. He’s patient, kind, and understanding. We went from having an open snack shelf to locking cupboards. His eating schedule has had to adapt to Bodhi’s. But it’s hard, finding balance between giving your child with T1D the attention they need, while still being fully present for your other child.
Breakthrough T1D Canada: What have you learned since those early days?
Kendra:
I’ve learned how important it is not to lean too heavily into toxic positivity. At first, I tried to “silver lining” everything. “At least we have CGMs, pumps, amazing doctors.” And it’s all true. But I also needed to leave room for honesty.
Through the lens of mental health, I’ve learned that it’s okay to say, “This sucks sometimes.” Bodhi doesn’t always want the attention that comes with being different; asking a parent to enter carbs when a friend offers a snack or navigating insulin doses at events. That constant spotlight can be hard for a kid.
And as a parent, it’s heartbreaking knowing there are parts of his experience I’ll never truly understand. But we sit with him. We let him tell us when it’s hard, when it hurts, when he’s frustrated. We don’t try to fix it, we just let him know it’s okay to feel that way.
In the beginning, I didn’t want to accept what it really meant to be his caregiver. The decision fatigue is real. Constant calculations: Is it hot out? How active will he be? What’s the carb ratio? When’s the next blood sugar spike? What’s the correction factor? These aren’t questions other parents have to ask themselves before heading out the door.
We give Bodhi permission to feel everything. To be disappointed. To be sad. We don’t downplay his experience. That’s not our right. And it wouldn’t help him feel any less alone.
Breakthrough T1D Canada: Any final thoughts you’d like to share?
Kendra:
We are so grateful for the research, the tech, and the medical teams that support us. These things do make managing T1D more possible than ever before.
But we take it one day at a time, with honesty.
(Somewhere in the conversation, Kendra receives a message from Bodhi’s kindergarten teacher.)
Kendra:
I saw the message and my heart jumped. It turned out another child had hit Bodhi on the shoulder. The teacher was just letting me know and had informed the other parents too. I took a breath and reminded myself, he’s upright, he’s okay, we’re winning today.
We’ve made major progress in the development of cell replacement therapies for type 1 diabetes (T1D) over the past few decades – much of it right here in Canada. We know that manufactured islets can be safely implanted into people, where they start to make insulin. But there is more work to do to advance these therapies to bring them to more people with T1D.
To drive new work in this area, Breakthrough T1D is pleased to announce a partnership with Canada’s Stem Cell Network (SCN), a non-profit, federally funded organization focused on stem cell and regenerative medicine research. Together, Breakthrough T1D and SCN will support four new projects led by Canadian researchers.
This announcement is an exciting expansion of a strategic partnership that began in 2021. In line with both organizations’ commitment to training future research leaders, we worked together to establish the J. Andrew McKee Fellowship program, awarded annually to a postdoctoral researcher working in regenerative medicine to join the Breakthrough T1D Centre of Excellence at UBC. Past fellows (awarded in 2022, 2023 and 2024) have brought expertise from many fields and countries to the Centre’s research team. Additionally, with both organizations’ interest in accelerating research to commercialization, Breakthrough T1D collaborated with Stem Cell Network to pilot a training program that aimed to increase the regulatory literacy of research trainees, which has subsequently reached many trainees working in regenerative medicine across the country.
To continue the increasing momentum in the field of stem cell-based therapies for T1D, we have now expanded our partnership to fund new translational research focused on innovation and commercialization. We are now excited to be able to announce four jointly funded projects that will receive support from May 2025 – April 2027. These grants are part of SCN’s 2025 national competition on regenerative medicine which is supporting a total of 36 grants.
Dr. Tim Kieffer (UBC), Dr. James Shapiro (University of Alberta), Dr. Takanori Takebe (Cincinnati Children’s Hospital), & Lunar Therapeutics (Vancouver, BC) – Fueling Biotechnology Partnerships Award
Combining stem cell-derived islets and vasculature for a better islet replacement product
Current cell therapies for T1D (i.e., islet transplantation), while often effective, are hampered by reliance upon donated organs and poor cell survival after transplant, necessitating large doses of cells and repeat procedures. This ambitious new project will address both the source of islet cells and the low cell survival rates associated with islet transplantation by accelerating Lunar Therapeutics’ pre-clinical development of a stem cell-derived islet replacement product, what Takebe’s lab describes as ‘complex miniature organs’ for T1D.
This product will consist not only of insulin-producing cells, but also endothelial cells – like those that line blood vessels and the heart. Endothelial cells will support islet cell survival and engraftment upon transplantation.
To accomplish this objective, Lunar Therapeutics will bring together Canadian expertise in stem cell-derived islets and clinical islet transplantation led by Drs. Timothy Kieffer and James Shapiro. The team will also include US-based Dr. Takanori Takebe who specializes in designing complex organoids composed of various cell types. Using technologies developed across each member’s laboratory, this multidisciplinary team will work to deliver an effective islet cell replacement solution.
Dr. Marya Ahmed & Dr. James Shapiro (University of Alberta) – Impact Award
Using naturally derived gels to optimize cryopreservation (extreme cold storage) of stem cell-derived islet
The implantation of stem cell-derived islets in people with T1D can restore insulin production, eliminating the need to inject insulin and improving the life quality of patients. However; after islet cells are harvested (from cadaveric donors) or created (from engineered stem cells) they must be stored before being used to treat a person with T1D. Currently, the storage and transportation of islet cells is difficult and the only storage method is freezing at low temperatures in the presence of reagents (chemical solutions) that help with the freezing process. However, these reagents cause cell death during thawing and can also cause allergic reactions in people when transplanted.
This project will address this gap in the field by aiming to develop non-toxic, naturally derived gels to optimize stem cell and islet freezing and storage. The identified gel-based products will be evaluated for commercial scale production. The success of this project will provide new intellectual property that will be of interest to researchers and companies in regenerative medicine in Canada and across the globe.
Dr. Corinne Hoesli (McGill), Dr. André Bégin-Drolet (Laval), Dr. Richard Leask (McGill), Dr. Andras Nagy (Sinai Health, Toronto), Dr. Steven Paraskevas (McGill) – Impact Award
Vascular lattice bioartificial pancreas for diabetes cellular therapy (Using blood vessels to create a better encapsulation device for islet replacement therapies)
Stem cell-derived islets offer a potentially unlimited source of islets for transplantation. Since stem cell-derived islets carry unique risks compared with donor-derived islets, containment within a device could allow retrieval if off-target growth ever occurs. However, encapsulation devices that have been tested in clinical trials so far and have shown minimal success, mainly because blood supply to the cells is limited within the devices. In this project, the team proposes to develop a device where the stem cell-derived islets are placed around pre-established vessels that can improve islet cell survival and speed of insulin responses via improved blood supply. In this project, they will optimize their device design and conduct advanced preclinical studies.
This project could lead to better survival and function of stem cell-derived islets. The device could provide long-term blood glucose control without external intervention. The project can also pave the way for other engineered human-scale bioartificial organs.
Dr. Megan Levings, Dr. Bruce Verchere, Dr. Francis Lynn & Dr. Peter Zandstra (UBC) – Impact Award
Using stem cells to create a human T1D immune system model in a petri dish
There are many new treatments on the horizon for T1D, such as replacement of insulin-producing cells, and therapies that seek to block autoimmunity, such as so-called “inverse vaccines” and immune cell therapies. However, a major barrier to all these therapies is the lack of an easy-to-use model in which their effects on human cells can be tested before advancing to human trials. The standard pre-clinical model is to test therapies in small animal models of T1D, but this has significant limitations since it is nearly impossible to replicate the human immune system. In fact, diabetes has been ‘cured’ hundreds of times in a mouse model, which has not translated to humans.
To overcome this barrier, Dr. Levings and her team will establish a new a model that recreates human T1D autoimmunity in the lab. The model will use stem cells to create the three types of cells that are involved in the disease: insulin-producing cells and two different types of immune cells, known as T cells and antigen presenting cells. Using the model, cells can then be combined in different ways to create a method that resembles what usually happens during autoimmunity.
A model of human T1D that can be generated in the lab will help test potential treatments and prompt new questions about why T1D develops, and how to prevent it. Thus, this research has the potential to support the further development of innovative therapies that may offer new approaches to prevent or treat people with T1D.
—
Curing T1D is the north star of Breakthrough T1D, and we are thrilled to continue to build upon and strengthen the relationship with SCN towards our shared goal of a world free from T1D through innovation and forward-thinking research.
Breakthrough T1D Canada will continue to provide updates on these projects as they become available.
Jim Beatty is a passionate volunteer in the fight against type 1 diabetes. For many years, Jim has volunteered with the JDRF, and now Breakthrough T1D, emceeing events and participating on various committees.
Jim has been living with type 1 diabetes for more than 20 years, following his adult diagnosis. Jim is a former journalist who now operates his own communications company in Victoria, B.C., where he likes to hike, fish and enjoy the West Coast with his family.
Breakthrough T1D Canada: Can you share what you remember about the lead up to you being diagnosed?
Jim Beatty: I was healthy, active; I had two young kids. At the time, I was the bureau chief for the Vancouver Sun covering the provincial legislature, which was a busy, stressful job. Every fall, I had my bloodwork done trying to get my cholesterol down. In the fall, everything was fine with my bloodwork. But things would soon change. As Christmas approached, I know exactly the morning – I was going to interview the Premier (Gordon Campbell at the time) for the usual year-end discussion, where we talk about the year that was, and year that will be, a kind of a state of the union address.
I remember I got dressed at home, put on my suit and tie but then saying to my wife that I don’t feel good, I don’t think I can go to work. I was so sick, and it hit me so fast that my wife had to call the press secretary to cancel the interview for me.
For two weeks, I had what I thought was very severe flu. But two months later, I noticed I was always exhausted, I would fall asleep after dinner, and I had an unquenchable thirst. I started needing to wake up in the middle of the night to use the bathroom. On their own, all these symptoms are all pretty benign and easily ignored or explained away.
But it wasn’t getting better, so I went to my family doctor, and he said let’s just do some bloodwork. Bloodwork came back and the doctor, said “you have diabetes.” Not type 1, just ‘diabetes’. I knew nothing about diabetes. Type 1 or two. Nobody had it in my family, I had no familiarity with this disease, and back then, there was no Google to look anything up.
I had an initial misdiagnosis of type 2, because when you were my age (36), for most doctors, they see it as most likely being type 2. I was told to modify my diet and do more exercise. I did all that, even though I had already been living that way before for the most part. I got my blood tested again and the A1C was still really high. They put me on Metformin, and that didn’t work either. And so, I needed to go insulin, with multiple daily injections.
I didn’t like needles, and I remember sitting on the side of my bed, with an actual needle and having to put that in my belly. I will never forget how tough that was, how invasive it felt. February was when I first told I had diabetes, and by summer I was on insulin therapy.
Breakthrough T1D Canada: How did you navigate your diagnosis?
Jim Beatty: I did everything the doctors told me to do; I didn’t foot drag on that. But I did feel robbed; I did feel that it might be a mistake (the diagnosis of T1D). I did think maybe I could exercise or diet my way out of it, maybe it’s a blip, a false-positive? I was doubting and I had persistent thoughts that I could work my way out of it. But after a while, it was quite clear it wasn’t going anywhere.
Unfortunately, I didn’t have anyone to talk to about it. I didn’t know anyone with type 1. Other than my family doctor, who I saw every 3-4 months, I was navigating it on my own. I wish that the supports that are available today were available then, especially for adults.
It was isolating, lonely, and there were just so many questions. Things that I take for granted now, I had no idea then. It was all new. I’d never handled a needle before. I’d never done finger poking (to check blood glucose levels). I certainly didn’t know what basal and bolus meant (types of insulins). My endocrinologist was talking in terms and language that I had no reference for. It was a confusing and frustrating period.
Initially, I was a newspaper reporter, and I did share with the two colleagues who I worked closely with, they needed to know I had this condition, that I might need sugar, that I was having frequent doctor’s appointments. I didn’t let management or bosses know, however. My thought process was that it was going to be an impediment to my career success, that it would be seen as a weakness, or a vulnerability. And that it might be a reason not to promote me to the next level.
Not long after my diagnosis, I moved to television broadcasting. I was the Bureau Chief with CTV Vancouver. I did tell the cameraman who I was working with every day, because for example if I told him I need to eat, I needed to eat. It wasn’t just hunger. It was a need.
But I still wasn’t comfortable with my diagnosis, and I didn’t speak freely, outside of family and friends.
I had moved my job again and I was the chief news anchor for CHEK News in Victoria, and this philosophy still hadn’t changed much. Bosses, news director, management – none of them knew I had type 1. I largely kept my diagnosis invisible. I would be anchoring the news, and when we went to commercial break, I had a little table next to me, and I would do a finger poke to see if I needed sugar, or to calibrate my insulin. And people didn’t know I was doing this; it was all hidden.
Then, a call from Breakthrough T1D (then JDRF), would change everything. I was asked to emcee a fundraising gala event. They were asking because I was a broadcaster and was known in the community, but they had no idea I had T1D. The request threw me into a bit of a tailspin because I knew if I was going to be genuine and host a fundraiser for type 1 diabetes research; it would be disingenuous not to admit I was also living with this.
I thought about the request for a few days. I ruminated over whether I should ‘go public’ and eventually I decided that yes, I’m going to do it. The first people I spoke with were my bosses. I said, ‘look I’m going to be hosting this event on Saturday, and it could be a news story when I reveal that I also have type 1 diabetes.’
Then, I stood up on the stage, and I basically ‘came out’ – ‘I am not just your emcee, I am one of you.’ And I told my story. It was a great night. It was a very liberating evening. People came up to thank me, I immediately felt support. And it was the beginning of being open about living with this disease and living with it as you need to. Unafraid to talk about it, being honest about any assistance you might need. It was a pivotal moment because it freed me.
I had no connection with Breakthrough T1D (JDRF) before that event, and it started a relationship that continues to this day. Galas in Victoria, Vancouver, Walks, Rides, government relations committee. It was very liberating and took me places I didn’t expect.
Breakthrough T1D Canada: What would a cure look like for you?
Jim Beatty: What I think of as a cure is something that will return my life to normalcy. Living without having to carry snacks with me, being hooked up 24/7 to the devices, being able to go for a walk or a hike, or to eat pizza, and not doing all the thinking and calculating that comes with it. A cure would be a life when I no longer have to constantly think about diabetes and all its complications. It would be a return to having the life I had before. So, yes, of course, it would be fantastic.
Five years, five years, every diabetic has said that they’ve been hearing ‘the cure is coming in five years’ for decades. That ‘five years’ is a false hope, so I don’t say that anymore, or believe it could be possible in five years.
So, when I think about the cure, I don’t think about the ‘cure’ per se. I am more interested in treatments today that are making my life better. And there are so many that I am using today that were pipe dreams twenty years ago. I am living my life better today because of the advancements in treatment, and those incremental things have made a significant difference. Today my A1C levels are better than they’ve ever been in my life, and that is because of the CGM and insulin pump, and how they help me manage my (blood glucose) levels more precisely.
A cure is a far-off, long-distance notion to me. I view treatments as real, closer, and more tangible.
Breakthrough T1D Canada: Is there anything else you’d like to share with the T1D community?
Jim Beatty: The thing I wish I had done was to be more open to these discussions, open about my diagnosis, earlier and not keep it a secret. By holding onto it, holding onto this big secret of something so significant in my life – at the time I thought it was the right thing. But now I know that’s not the case. I could have learned more, had more support, my journey would have been better and easier, much sooner.
So please know that you don’t need to feel isolated. You can be open; you can reach out for assistance. Take the help. And know that life is good today.
We are pleased to announce 6 new grants funded via Breakthrough T1D International (USA) to stellar Canadian scientists. These grants all support cell therapy research to replace insulin-producing cells in people living with T1D.
Dr. Cristina Nostro, University Health Network (Toronto)
To date, global efforts on this work – largely led by Canadians – has used research-grade cell lines which are less expensive and more readily available for experimentation. To move these therapies towards the clinic there is a requirement for Good Manufacturing Practices (GMP) to be met. This includes properly trained personnel, GMP-certified premises and equipment, clinical-grade starting cell lines, validated protocols and practices, etc.
Two shots on goal: These two grants will each use Dr. Nostro’s world-renowned differentiation protocol to engineer islets using clinical-grade stem cell lines in GMP-certified facilities that have the ability to scale up the differentiation process.
Consider Dr. Nostro’s differentiation protocol as an excellent sourdough bread recipe perfected in her kitchen with consistent, delicious results. That recipe will now be taken to two different commercial bakeries to use their ingredients and facilities to see if they can make the same excellent sourdough loaves consistently in large production quantities.
Dr. Guy Rutter, CHUM Montreal
Imaging to explore the survival and function of stem cell-derived islets transplanted in mice
Goal: A novel imaging technique to examine human stem cell-derived islets in mice
Will allow real-time comparison of transplant sites (liver vs under skin)
Better assessment of cell death / blood supply / immune attack
A significant hurdle for assessing T1D and islet transplantation is that there is virtually no way to ‘see’ islets inside a person, even in small animals. No imaging technique allows us to ‘look at islets’ and see how many are alive, functional, producing insulin, etc. This is why some clinical trials using islet transplantation devices (microencapsulation) have involved device removal at periodic timepoints so that the islets can be removed from the body and examined to evaluate their survival and function. Dr. Rutter is proposing a novel imaging technique to ‘see’ islet functioning in mice, which can help guide factors affecting the survival and function of transplanted islets.
Dr. Patrick MacDonald, University of Alberta
Artificial Intelligence (AI)-driven benchmarking for understanding and improving stem cell-derived islets
Over the past 5+ years, Dr. MacDonald and his team have created a groundbreaking database: humanislets.com, which isolates islets from donated pancreases (from deceased donors with T1D, T2D, and without diabetes) and characterizes the islets and their function using “omics”. This is a broad term to encompass the study of all the biological molecules of a cell, such as genomics (DNA), transcriptomics (RNA), proteomics (proteins), and metabolomics (metabolites), etc. Together “omics” data creates an exceptionally robust characterization of each islet – and all of this is made publicly available to scientists around the world through this research.
Goal: Dr. MacDonald’s new grant will expand this Breakthrough T1D-funded database to include stem cell-derived islets for comparison to donor islets and incorporate artificial intelligence methods to dig deeper into this comparison.
Dr. Haoning Cen, University of British Columbia
Postdoctoral Fellowship(Supervisors: Dr. Francis Lynn & Dr. Leonard Foster)
A blueprint for making better beta cells
Goal: to create blueprints for donor beta cells vs stem cell-derived beta cells
Will use protein detection to identify 10,000+ proteins
Will classify each protein’s quantity and location to compare ‘natural’ vs stem cell-derived beta cells
Biomaterial platform for islet transplantation under the skin
Goal: to create a biological scaffold (a small structure made from bio-compatible materials that can support new cell growth and survival) for islet transplantation using regenerative hydrogel.
The scaffold will support blood vessel, nerve, tissue growth to support islet survival
Immunomodulating therapy (modifying the immune system’s function, for example) embedded in the scaffold will be explored
Type 1 in year 1: turning the page on an unexpected diagnosis at university
Meet Aryssah, an incredibly resilient adult living with type 1 diabetes (T1D). She is a committed $100M Campaign to Accelerate volunteer and champion of diabetes and mental health support. She devotes her time to appreciating the incredible philanthropic donors who help fuel Breakthrough T1D’s Mental Health Strategy for Type 1 Diabetes. She also generously funds ascholarship for students with T1D attending their first year of university.
This Mental Health Awareness Month, Aryssah candidly shares her T1D journey to spread awareness of the daily burdens endured by those living with this autoimmune disease. Her story paints a stark picture of the gaps in diabetes care and support in Canada, particularly for newly diagnosed adults—gaps we are working to address with donor support.
Nearly 300,000 Canadians live with T1D today, with approximately 12,200 diagnoses anticipated in 2025 alone. $100M Campaign to Accelerate donors play a significant role in speeding up a future where everyone with T1D has access to the care, tools, and resources they need to thrive.
Had Aryssah received comprehensive support at diagnosis—addressing not only the physical demands of T1D but its mental tolls, too—her early years with T1D may have looked different. But like many impacted by T1D, Aryssah does not let her diagnosis, or this disease, stop her from courageously pursuing a hopeful and fulfilling life. Aryssah shares her story with candour and the utmost care for the T1D community, hoping to garner even more support to improve lives and accelerate cures.
When Aryssah was 19, she became lethargic and would get foot cramps after sports, which was unusual for a young varsity athlete. With additional symptoms like increased thirst and significant weight loss, she was diagnosed with T1D shortly after a visit to her family doctor.
Had she been diagnosed just one year prior, she would have gotten support and resources through the pediatric diabetes clinic. Instead, she was treated like an adult and had to figure out how to manage this autoimmune disease on her own. She remembers going to the diabetic nurse’s office only to be given a couple of insulin pens and have them prick her finger. “It felt very independent,” she says, “in reflection now, part of me is a little sad for myself at that time, because if I was diagnosed a couple of months earlier, I would have been set up at SickKids and would have been walked through the whole process with my mom.”
Initially, Aryssah didn’t feel that T1D was too severe. As an active young adult, she felt invincible. She even ran a marathon just a mere three months after being diagnosed. But for the first few years living with T1D, she struggled to navigate her new reality. She found it challenging to balance such a complex disease while attending classes, competing as an athlete, and wanting to participate in the entire university experience.
Ill-equipped to properly manage her blood glucose levels, she was in and out of the hospital throughout school and, as a result, unable to finish her fourth year. These hospitalizations were very traumatic for her, and overall, she didn’t feel like herself.
“I did not take care of myself in the way that I should have. And it’s probably because I didn’t have that support in the beginning to set me up for success down the road,” she says.
In her mid-twenties, she sought out a psychotherapist to figure out how to deal with these traumas and the mental health aspects of living with T1D. Therapy allowed her to process and accept her diagnosis and has been integral to her health journey ever since. Perseverance and optimism are in her nature, and she has always used her diagnosis as fuel to combat adversity.
Later in life, when Aryssah could better manage her blood sugars, she returned to school and completed her university degree with Honours. For all those living with T1D or newly diagnosed, she advises, “This is one instance of your health where you have to relinquish control almost automatically because you can do everything right (you can track your carbs and can inject what you need to), and your blood sugar’s still going to muck up; it’s not a science…We are all trying our best and are so much larger than our actual diagnosis or disease.”
Through Breakthrough T1D, Aryssah also developed meaningful connections with the T1D community. Having support from those who understand the disease firsthand has been invaluable to her. As a form of giving back, Aryssah established the Torchbearer Scholarship for Type Ones to help support others navigating the highs and lows of T1D while attending university. All students who live with T1D entering their first year of university are invited to apply for this $1,000 scholarship opportunity. The application deadline is July 31, 2025, at 11:59 p.m. EST.
“You cannot see the destruction that diabetes does to your brain as a young adult or even as you continue to grow,” Aryssah says, “and that is sometimes even more important than blood sugar management because it goes hand-in-hand. Mental health is something that we need to take into consideration. It never really comes up with diabetes.”
$100M Campaign to Accelerate donors are speeding up progress to ensure that no one is left to manage this disease alone, as Aryssah and countless others have had to.
Peter Dreimanis is a multidisciplinary artist, perhaps best known as a co-founder of the Juno Award-winning band July Talk.
In June 2020, he was diagnosed with type 1 diabetes (T1D) as an adult and had to learn to navigate the disease against the backdrop of lockdowns and uncertainty of the pandemic.
Peter recently sat down with Breakthrough T1D Canada to share his story of being diagnosed later in life, and how T1D has changed his life as an artist, partner and father.
Breakthrough T1D Canada: Tell us a little about when you were diagnosed.
Peter: Well, I got COVID at the very beginning of the pandemic. We’d been touring as a band for the better part of 12 years or so, and I was never someone to listen to my body. I didn’t have the skills to know what my body needed, to determine if something was wrong. I was better at silencing things – driving through pain, ignoring the signals to slow down etc.
A while before the pandemic shutdown, in January of 2020, my partner bought tickets to see my favourite team play in Buffalo. We went across the border and when we came home, we got incredibly sick, worse than I have ever been. It was an extreme illness. You know what a flu bug feels like, but I wasn’t plugged into the scientific news, wasn’t paying attention to the slowly emerging news about covid. So, all this to say, I got very sick for a couple weeks, and then slowly we approached the shutdown.
Around April, I started having people say I ‘looked great’, I looked like ‘I had been working out, lost weight’ – and I didn’t know what to make of it. One of my roommates was vegan, I’d been eating those meals, not going out for food, but I wasn’t really making lifestyle choices.
And always, I continued to just push through. I didn’t pay it much thought until around May/June – I was experiencing extreme thirst, I was eating ice cream, eating giant meals of sourdough bread and rice, and still I was losing weight.
I attributed it to being a workaholic in a state struggling to accept that we had to slow down. We (July Talk) had been working on an album. I was in denial, and still just trying to make the album work.
And I continued to worsen, I would have days where I would be drinking 10-12 litres of water a day, I couldn’t get enough. I would walk up the stairs with equipment and think I would pass out. We did huge shows in summer 2020, we put together a socially distanced concert experience, drive-in and broadcast at the drive in. It was a massive undertaking; I worked full-time for 3 months to try and figure out how to pull it off. So, I was laser focused on that. And I remember I would go down for a nap at like 6pm, so exhausted I couldn’t think, and I wouldn’t wake up until the next morning. I was just so exhausted, so thirsty, so confused.
And yet – it wasn’t until a professional photographer took some photos to help promote the show that I realized, wow, I look really skinny. I weighed myself and I was 50lbs lighter. My partner had been on me about how thin I was looking. You could see my ribs. I had no frame of reference; I had never been rewarded for slowing down. But thank goodness I went and got blood tests and was immediately diagnosed – first with type 2.
I was initially put on metformin, and it obviously didn’t work. I fortunately was seen by an endocrinologist who immediately recognized it as type 1. So, I went on insulin therapy, and I still see this same endo today. I was connected with a DEC (diabetes education coordinator), and a nurse. I was weeks away from this show. They warned me that if I didn’t take this on (managing my T1D), I could die. My partner was and has been incredible, And I realize now how much T1D affects the people who love you. I harbour some shame and guilt around my will to take it on; for not truly recognizing, or perhaps accepting, the severity of the situation.
I did my first insulin shot two or three days before we went on stage, and I really didn’t know what I was doing. I was using fingerpricks (to measure blood glucose levels) at the time. I wasn’t taking it seriously right away. It’s truly a continuous lifestyle change, and I don’t think I really understood the gravity of that yet. I got through the shows somehow without going low. My adrenaline seems to send me up. In my experience touring since diagnosis, I always have juice on stage. I’m always going on stage at around 9 (blood glucose level) – my adrenaline has the opposite effect. So, when the adrenaline crashes, that’s when I need the fast-acting carbs.
As soon as this show was done, I went north of the city (Toronto), turned off my emails and phone, did Zoom calls and really started to learn what it means to live with type 1 diabetes.
Breakthrough T1D Canada: How have you adapted since then to your new normal with T1D?
Peter: I felt so supported. I was totally floored by the system that springs into action, I would have rather it be in person instead of over Zoom etc., but it was absolutely stunning how quickly they were able to get us up to speed. Once I was ready, I made every effort to learn how to carb count, etc., – I had notebooks full of stuff. It really takes a while to learn. I liken it to when you’re a new driver and the insurance company tells you that you ‘will get in an accident’. My T1D ‘accident’ was that I had a low (hypoglycemic episode) that resulted in a grand mal seizure, and it was just miscounting my carbs, there was more learning to do. I didn’t know then what I know now.
When it happened, I was on a long phone call with my parents, and I started feeling sweaty and shaky. By the time I was trying to get juice, I was reading at 2.4 (a very low blood glucose level). And by then it was too late, and I went into seizure.
It was a horrifically traumatic experience for me and my family. For a while after, I had panic around lows. I definitely accepted going higher for about a year after that, because of how scary that experience was. I felt like a ticking time bomb that could explode at any minute. All you have to do is look into your partner’s eyes to know how scary it was for them. But knowing that danger gave me a better understanding of what the body experiences when it goes low, and what it actually means to live with this chronic condition. I can handle a low now. But it took time to have the clarity to understand it wasn’t going to be like this forever. And I had some consequences from that episode, like not being able to drive for six months, losing trust in my body etc. But I see it now as a profound life experience, and I grew up a lot.
To speak more about the balance of it, and this is something I give a lot of thought to, we are all simply by waking up in the morning, we are all in a place of trusting our bodies to function as we think they should do. Our bodies are one of the most complex systems in existence, and the pancreas producing insulin, and all the rest of our parts doing what they should do – we never truly think about it. It’s an incredible privilege, the way we think we’re going to be okay is by believing we will be OK.
And for those of us with T1D, that might take technologies, or therapy or whatever you need to rebuild that trust. We have a contract with our bodies, and sometimes I think about it, like when we’re running down a street, there are moments when we’re airborne. And we trust that we’ll land. And I think about how to keep that trust and cultivate that trust in your body. Because it’s the only way we can get through life. And now as someone with T1D, I need to spend more time building that trust because it’s the only way to be OK.
Breakthrough T1D Canada: What T1D research excites you the most right now?
Peter: I don’t consider myself a fully informed person on T1D research, but I’ve read about smart insulins that might eliminate carb counting, and this intrigues me. To free myself of that constant testing (blood glucose levels), to no longer live in a world where you must understand everything you’re eating, to be precise about insulin against that. In a restaurant it’s a guessing game (how many carbs are in a meal). Life doesn’t work that way, in exacts. When you live an untraditional lifestyle, I’m not in a 9-5 job, I’m a parent, sometimes I want to eat my kids’ leftovers without having to calculate percentages.
I say godspeed to the researchers who might be able to eliminate the 10K thoughts I have in a day. Not thinking that much, that would be freedom that I can’t comprehend, and I think especially about people who have lived with T1D for most of their life. It would be incredible. I eagerly await this. I feel very grateful for my CGM and insulin pump, and in all honesty, they drive me nuts, a lot of the time I hate it, but also feel lucky in that I have only experienced T1D when this tech exists, in this unbelievably progressive time. I don’t take that for granted at all. I feel lucky in that way.
Breakthrough T1D Canada: Do you have any last thoughts to share with your fellow T1D community?
Peter: Having the opportunity to hear other people share so openly and honestly as part of the Beyond the Numbers video project turned out to be more helpful than I could have realized before we started.
Talking with others is so therapeutic, none of us are perfect, and we will have many hard and challenging days and times living with T1D. I encourage people to be kind to themselves, to share as much as they are comfortable when things are hard, and to reach out for support when it’s needed. It’s a journey, and there will be bumps along the path, but the support is there.
May is Mental Health Awareness month, a national movement to raise awareness of the importance of mental health and the structural gaps that exist in accessing treatment and support.
Mental health is central to living well with type 1 diabetes (T1D). This is why, in 2021, Breakthrough T1D Canada launched its Mental Health Strategy, with the goal of better supporting mental health in people with T1D, while we continue to support research towards cures.
T1D affects a person’s emotional, social, and mental wellbeing throughout their lifetime, known collectively as psychosocial health. Psychosocial challenges can negatively impact diabetes outcomes like glycemia. Many people with T1D experience “diabetes distress” – a term describing the powerlessness, stress, guilt, relentless worry and denial that accompanies living with diabetes and the burden of self-care. In addition, people with T1D are at higher risk of mental health disorders including depression, anxiety and disordered eating. These challenges are common in people with T1D and can be treated – but they are often underappreciated or undertreated because of gaps in care and support.
To better address these areas of need, Breakthrough T1D outlined a three-pronged approach to its Mental Health Strategy: 1) knowledge generation through new research, 2) a new training program for mental health providers, and 3) development of new community supports. Since 2021 when we laid the foundations of this strategy, we have driven substantial progress in all three key areas, thanks to the generous support of donors, as well as partnerships with academia, other diabetes organizations, and community collaborators.
We are pleased to share the updates to this program that have taken place in the past year.
This includes funds from Breakthrough T1D Canada, Brain Canada, CIHR, and MSFHR
9 awards total:
3 with Brain Canada
4 with CIHR
1 impact award (BT1D only)
1 partnered award to Dr. Tricia Tang (Michael Smith-Health Research BC)
All the new research funded is still in progress. In line with our global research strategy in this area to build programs that are designed to scale up and ultimately help larger numbers of people, many of the projects we are supporting involve development and testing of digital interventions. For example, Dr. Tricia Tang and her team at the University of British Columbia (UBC) carried out a clinical study of their virtual peer support platform called REACHOUT. This platform uses a mobile app to deliver peer-led mental health support by trained mentors to adults living with T1D in rural and remote regions of BC. The trial assessed the effects of virtual peer support on outcomes including diabetes distress, quality of life, and HbA1c. Future work will focus on iterative improvement of the REACHOUT platform and scaling up the reach of trained mentors so that more people with T1D can be supported.
Other studies that are leveraging digital technologies to engage people with T1D across Canada include that of Dr. Deborah Da Costa at McGill University, whose study is testing how best to support the mental health and wellness of women with diabetes during pregnancy, and that of Dr. Holly Witteman from the University of Laval, who is developing a network of virtual peer support for people with T1D with specific needs and interests.
Other Breakthrough T1D-supported research is focused on improving outcomes around the transition from pediatric to adult care, a life stage when many youth stop seeing their endocrinologist, which can lead to challenges such as rising HbA1c, isolation, stigma, and eating disorders. Dr. Sonia Butalia at the University of Calgary is carrying out a clinical trial of a system designed to improve this transition, which saw improved blood glucose levels among those involved in the program’s initial pilot in Calgary. In the latest trial funded by Breakthrough T1D and CIHR, the program, which consists of a transition coordinator and carefully designed communications, is being scaled to other Alberta Health Services (AHS) sites in Calgary, Edmonton, Lethbridge, Medicine Hat, and Red Deer.
These clinics and community partners are very keen on the team’s transition work, and AHS has approved the budget for this project to be sustained past the life of the grant. Translation of this work would mean that this demographic of people living with T1D will no longer fall through the cracks during the transition from pediatric to adult care.
“My son Luke has lived with T1D since he was 5 years old, and now he is a teenager. It has been a big challenge for him and our whole family, and though Luke is well-supported, in large part due to his involvement with Breakthrough T1D, adolescence and early adulthood bring a whole new set of challenges. I am so glad Dr. Butalia and her team are implementing a model of transition-age care that hopefully will be able to help Luke in a couple of years. It’s great to see this vital research being scaled across Alberta and ideally expanded across the country.” -Ryan MacDonald, Calgary, Breakthrough T1D Campaign to Accelerate Co-Chair.
Mental Health + Diabetes Training Program
Many people with T1D face mental health challenges that require the support of a registered mental health provider – ideally one who understands the unique mental health challenges posed by diabetes. To help inform Canadian mental health providers about diabetes, Breakthrough T1D launched the Mental Health + Diabetes Training Program in early 2023, in collaboration with Diabetes Canada.
This fully bilingual course is offered virtually as two streams: one for registered Canadian mental health providers (which includes a live facilitated session focused on clinical competencies), and one for other healthcare providers and the public that consists only of self-guided modules. The course is delivered at no cost, provides 10 Continuing Education credits for selected providers, and has been approved by the Canadian Psychological Association as well as other associations.
As of May 2025, over 500 mental health providers have completed the program thus far, and over 1000 others (other types of healthcare providers, or members of the T1D community) have enrolled in the training. Early outcomes of the training program’s impact have recently been published as a peer-reviewed paper in the Canadian Journal of Diabetes. An additional evaluation study is in progress that will assess the impact of the program on trainees’ clinical practice.
Development of Community Supports
The T1D community is diverse and includes many subgroups with varying psychosocial needs and challenges. Towards meeting this need, in the first three years of our strategy, we strove to develop community supports through several different activities, with the help of our dedicated Mental Health Advisory Council—a group of >100 volunteers with diverse lived experience of T1D. In the past year, we continued to expand our sources of community support in a number of ways.
First, we delivered several virtual events to engage and educate our community:
Over 500 individuals attended our Breakthrough T1D Education Series – T1D and Mental Health sessions in May 2024 (in English and French).
Nearly 200 healthcare providers attended sessions on T1D and eating disorders (in English and French) hosted in collaboration with the National Eating Disorder Information Centre (NEDIC). These webinars helped increase dialogue and learning opportunities for healthcare providers and others.
Over 500 people attended our Breakthrough T1D Education Series – Disordered Eating and T1D. These bilingual events featured speakers from NEDIC, ANEB (Anorexie et boulimie Québec), and people with lived experience and explored the realities and challenges of managing T1D-related eating disorders. By fostering dialogue on this underappreciated topic, we hope to see eating disorders recognized and treated more effectively, leading to better care and outcomes for those impacted.
Second, we expanded our Directory of mental health providers who have been trained in diabetes through our new training program, as a resource for people with diabetes or healthcare teams to connect with a mental health provider with knowledge of their disease. As of May 2025, we list >180 providers from across Canada and anticipate that listings will grow over time as more providers are trained.
Third, we monitored progress and facilitated the success of projects funded through our inaugural Mental Health and T1D Community Grants program, a mechanism to catalyze the efforts of other organizations to develop new community-facing programs designed to support and improve mental health and wellness in the T1D community. The first grants awarded through this program are progressing well through their 18-month term, and updates will be provided upon their conclusion in late 2025.
Finally, we are pleased to share a new video series to share stories from our community: Beyond the Numbers: Real stories of navigating mental health with T1D. We will be sharing these videos throughout Mental Health Awareness Month and beyond, to help normalize the psychosocial problems, solutions, and wins that are part of daily life with T1D. Featuring 20 videos, this series addresses themes of Relationships and Social Support, Life Transitions, and Coping and Resilience.
Thank you to our community
Breakthrough T1D Canada remains enormously grateful for the support of our Mental Health Advisory Council, lead volunteers and philanthropic partners, including funding partners Brain Canada and Diabetes Canada, without whom our progress in this area would not be possible.
To mark the start of Mental Health Awareness Month, Breakthrough T1D Canada is excited to launch its new video series Beyond the Numbers: Real stories of navigating mental health with T1D that focuses on sharing the real stories of people living with type 1 diabetes (T1D).
The idea for the video series began in October 2023, when Breakthrough T1D was approached by multidisciplinary artists Michael Pivar and Peter Dreimanis with a vision: to capture real stories from people living with type 1 diabetes, exploring how T1D affects their mental health and emotional well-being. The concept was compelling—intimate interviews that didn’t shy away from the harder conversations, and that focused on lived experience, not clinical advice.
At the same time, Breakthrough T1D had just wrapped up a round of focus groups with Breakthrough T1D’s Mental Health Advisory Council who indicated that adults living with T1D were interested in video content from “people like them” about the day-to-day mental health/wellness concerns related to T1D.
Based on their feedback, three themes for this video series were identified:
Relationships and Social Support
Life Transitions
Coping and Resilience
Over the course of a year, five adults, Christine, Lujane, Meagan, Rodrigo, and Tracey—were interviewed. Their conversations touch on stigma, including changing the conversation around diabetes devices, disordered eating and diabulimia, relationship challenges, being diagnosed in adulthood, and their own personal coping strategies.
Each person shared openly and with vulnerability, with the hope that their stories might help others feel less alone. The goal was to normalize conversations around the mental health impacts of T1D and to shine a light on the emotional side of this often invisible illness—because the challenges are real, and deserve to be acknowledged.
Breakthrough T1D is extremely grateful to Christine, Lujane, Meagan, Rodrigo, and Tracey for their openness and willingness to share. We would also like to extend our heartfelt thanks to Mike Pivar and Peter Dreimanis—without their creativity, dedication, and care, this project would not have been possible.
We hope that Beyond the Numbers not only sparks connection and empathy, but also inspires future dialogue—at home, in healthcare settings, and across the wider community.
National Volunteer Week takes place from April 27 – May 3, 2025, as organizations across the country celebrate those who generously donate their time and talents to their communities and for causes close to their heart.
The National Volunteer Week theme for 2025 is Volunteers Make Waves. In the words of Volunteer Canada this theme: Highlights the power, impact and importance of individual and collective volunteer efforts across Canada. Like a wave, volunteering is movement building.
Water is in constant motion, always flowing, shifting, and transforming with every powerful wave or quiet ripple. And so is each volunteer’s contribution toward creating impact in our communities.
Each individual volunteer contribution, big or small, creates momentum and has the power to influence and inspire, joining a wave of positive change.
This theme resonates throughout the story of Breakthrough T1D. We were founded by a group of devoted parents determined to find a cure for their children living with type 1 diabetes (T1D), and through their contributions, momentum continued to grow, creating tremendous progress in improving everyday life with T1d and bringing us ever closer to cures for this disease.
For the past three years, it has been our honour and privilege to celebrate our amazing volunteers and their support of the T1D community through our Annual Volunteer Awards.
In 2024 we were thrilled to recognize individuals, volunteer committees and corporate organizations who have demonstrated incredible commitment, devotion and heart in supporting our collective goal of a world one day free from T1D.
Our volunteers are the foundation of everything we do, and we are thrilled to share with you the 2024 Breakthrough T1D Canada Volunteer Award Winners.

















 Kendra Fisher is a former member of Team Canada’s hockey program, a 3x world inline hockey champion, and a firefighter. She is also the Founder of Mentally Fit; a professional speaker, a mental health coach, and an author in the making. Kendra may be best known for her hockey career, and for making the life-altering decision to step away from her dream of playing for Team Canada in order to manage diagnoses of Generalized Anxiety Disorder, Panic Disorder, Clinical Depression, Agoraphobia, and OCD.
Kendra Fisher is a former member of Team Canada’s hockey program, a 3x world inline hockey champion, and a firefighter. She is also the Founder of Mentally Fit; a professional speaker, a mental health coach, and an author in the making. Kendra may be best known for her hockey career, and for making the life-altering decision to step away from her dream of playing for Team Canada in order to manage diagnoses of Generalized Anxiety Disorder, Panic Disorder, Clinical Depression, Agoraphobia, and OCD. The surreal part was that those were the only symptoms; excessive thirst and urination. He was otherwise his normal, happy, outgoing self. They got him on an IV right away and started titrating insulin. It was all happening so fast, trying to understand what was going on while still in complete shock.
The surreal part was that those were the only symptoms; excessive thirst and urination. He was otherwise his normal, happy, outgoing self. They got him on an IV right away and started titrating insulin. It was all happening so fast, trying to understand what was going on while still in complete shock. Through the lens of mental health, I’ve learned that it’s okay to say, “This sucks sometimes.” Bodhi doesn’t always want the attention that comes with being different; asking a parent to enter carbs when a friend offers a snack or navigating insulin doses at events. That constant spotlight can be hard for a kid.
Through the lens of mental health, I’ve learned that it’s okay to say, “This sucks sometimes.” Bodhi doesn’t always want the attention that comes with being different; asking a parent to enter carbs when a friend offers a snack or navigating insulin doses at events. That constant spotlight can be hard for a kid.

 Initially, I was a newspaper reporter, and I did share with the two colleagues who I worked closely with, they needed to know I had this condition, that I might need sugar, that I was having frequent doctor’s appointments. I didn’t let management or bosses know, however. My thought process was that it was going to be an impediment to my career success, that it would be seen as a weakness, or a vulnerability. And that it might be a reason not to promote me to the next level.
Initially, I was a newspaper reporter, and I did share with the two colleagues who I worked closely with, they needed to know I had this condition, that I might need sugar, that I was having frequent doctor’s appointments. I didn’t let management or bosses know, however. My thought process was that it was going to be an impediment to my career success, that it would be seen as a weakness, or a vulnerability. And that it might be a reason not to promote me to the next level.
 Postdoctoral Fellowship (Supervisor: Dr.
Postdoctoral Fellowship (Supervisor: Dr. 
























