We use cookies to enhance your browsing experience, serve personalized ads or content, and analyze our traffic. By clicking "Accept All", you consent to our use of cookies.
Customize Consent Preferences
We use cookies to help you navigate efficiently and perform certain functions. You will find detailed information about all cookies under each consent category below.
The cookies that are categorized as "Necessary" are stored on your browser as they are essential for enabling the basic functionalities of the site. ...
Always Active
Necessary cookies are required to enable the basic features of this site, such as providing secure log-in or adjusting your consent preferences. These cookies do not store any personally identifiable data.
Cookie
cookieyes-consent
Duration
1 year
Description
CookieYes sets this cookie to remember users' consent preferences so that their preferences are respected on subsequent visits to this site. It does not collect or store any personal information about the site visitors.
Functional cookies help perform certain functionalities like sharing the content of the website on social media platforms, collecting feedback, and other third-party features.
Cookie
_dc_gtm_UA-*
Duration
Less than a minute
Description
Google Analytics sets this cookie to load the Google Analytics script tag.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics such as the number of visitors, bounce rate, traffic source, etc.
Cookie
_gcl_au
Duration
3 months
Description
Google Tag Manager sets the cookie to experiment advertisement efficiency of websites using their services.
Cookie
_ga
Duration
1 year 1 month 4 days
Description
Google Analytics sets this cookie to calculate visitor, session and campaign data and track site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognise unique visitors.
Cookie
_gid
Duration
1 day
Description
Google Analytics sets this cookie to store information on how visitors use a website while also creating an analytics report of the website's performance. Some of the collected data includes the number of visitors, their source, and the pages they visit anonymously.
Cookie
_gat_gtag_UA_*
Duration
Less than a minute
Description
Google Analytics sets this cookie to store a unique user ID.
Cookie
_ga_*
Duration
1 year 1 month 4 days
Description
Google Analytics sets this cookie to store and count page views.
Cookie
_gat_UA-*
Duration
Less than a minute
Description
Google Analytics sets this cookie for user behaviour tracking.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
No cookies to display.
Advertisement cookies are used to provide visitors with customized advertisements based on the pages you visited previously and to analyze the effectiveness of the ad campaigns.
National Volunteer Week takes place from April 27 – May 3, 2025, as organizations across the country celebrate those who generously donate their time and talents to their communities and for causes close to their heart.
The National Volunteer Week theme for 2025 is Volunteers Make Waves. In the words of Volunteer Canada this theme: Highlights the power, impact and importance of individual and collective volunteer efforts across Canada. Like a wave, volunteering is movement building.
Water is in constant motion, always flowing, shifting, and transforming with every powerful wave or quiet ripple. And so is each volunteer’s contribution toward creating impact in our communities.
Each individual volunteer contribution, big or small, creates momentum and has the power to influence and inspire, joining a wave of positive change.
This theme resonates throughout the story of Breakthrough T1D. We were founded by a group of devoted parents determined to find a cure for their children living with type 1 diabetes (T1D), and through their contributions, momentum continued to grow, creating tremendous progress in improving everyday life with T1d and bringing us ever closer to cures for this disease.
For the past three years, it has been our honour and privilege to celebrate our amazing volunteers and their support of the T1D community through our Annual Volunteer Awards.
In 2024 we were thrilled to recognize individuals, volunteer committees and corporate organizations who have demonstrated incredible commitment, devotion and heart in supporting our collective goal of a world one day free from T1D.
Our volunteers are the foundation of everything we do, and we are thrilled to share with you the 2024 Breakthrough T1D Canada Volunteer Award Winners.
From years of burdensome insulin injections to the insulin pump that saved her life.
Lynn Cameron is a passionate advocate at Breakthrough T1D, fiercely pursuing positive change for Quebec’s type 1 diabetes (T1D) community, which desperately requires public coverage of T1D devices. Lynn has lived with this autoimmune disease for nearly 60 years, many of which she endured without access to the advanced technology she needed to thrive. Over the past five decades in her T1D journey, she has overcome countless obstacles, compounded by the burden of self-advocacy for the care she deserves.
Lynn is 63 years old, and due to Quebec’s age restriction on its public coverage (only available to those who enroll in the program under age 18 and are then covered for life), she and over 40,000 adults in her province do not qualify. This creates inequity among Quebecers living with T1D merely based on their age of diagnosis. No individual living with T1D should suffer because of their age or geographical location. That’s why Lynn continues to stand up for all those living with T1D, determined to ensure no one else goes through what she has. She hopes her story can help others and inspire critical change.
Lynn doesn’t remember life before type 1 diabetes. “It’s been so many years; I don’t count anymore. I don’t remember not being diabetic. I was young. The only thing I remember was the first insulin shot my father gave me,” she says.
In 1967, at the time of Lynn’s diagnosis, diabetes technology and care were vastly different than they are today. Insulin syringes were only available in whole-unit increments rather than half-units. This meant less control over how much insulin she could administer, leading to increased blood glucose fluctuations. The insulins also kept changing, and Lynn says she was allergic to one which is no longer on the market today. Dieticians were not part of diabetes care, even though carb counting and knowing how different foods impact blood glucose are essential for T1D management. All these factors made life with T1D difficult for Lynn.
“When I was diagnosed, I was told that you have to be careful about what you eat and have to be active and do everything correctly,” Lynn says, “I was always up and down [blood glucose levels], and it was not because I was not doing or watching what I was supposed to do.”
These challenges fluctuated over the years, after a difficult childhood, adjusting to life with T1D and undergoing heart surgery at the age of 10. As an adult, Lynn relished any opportunity to be active outdoors until diabetes complications started taking a toll on her health.
In 2012, Lynn began trying to get an insulin pump to improve her quality of life after enduring multiple daily injections (MDI) for 45 years. She tried hard to convince the RAMQ, Quebec’s government health insurance board, to cover pumps. It wasn’t until 2021, after nine years of self-advocating, that Lynn finally received her insulin pump, covered until December 2025—not by her own government but by donors to a hospital foundation.
“When I got the insulin pump, things did change so much, and I got better,” Lynn says. Since being on the insulin pump, her blood glucose levels have improved significantly.
Recently, this technology also allowed her to receive a second heart surgery, without which she would not be alive today. Doctors don’t always allow patients to wear insulin pumps during surgery, making this a significant step in diabetes care in Quebec. After waking up from the operation, Lynn was shocked to see her blood glucose stable. She asked the doctor what he did, and he said that the insulin pump, her external organ, did all the work. “That was a gift of life,” Lynn says, “because if I wouldn’t have been on the insulin pump, they wouldn’t have operated, and I wouldn’t be here.”
This is why advocating for access to life-saving devices is so close to Lynn’s heart. She says, “It’s 2025; it shouldn’t be like this. That’s why I’m doing what I can to work with Percée DT1 [Breakthrough T1D] and giving my time because of their mission. I think that insulin pumps will be temporary for about 10 years, and then probably there’s going to be a cure.”
Lynn’s incredible efforts include meeting with elected Members of the National Assembly (MNAs) of the official opposition in Quebec to share her story and lobby for adult coverage of insulin pumps for herself—she refuses to return to MDIs when her funding expires—and thousands of other Quebecers. She communicated the burden of MDIs, such as requiring 21 needles every three days compared to one with the pump, and the increase in daily decisions, which can lead to more errors in T1D management. Lynn is voicing her right to live, letting the province know that this situation undermines her integrity and dignity. She also supported Breakthrough T1D’s letter-writing campaign, helping acquire signatures of support from local MNAs.
Lynn’s resilience, tenacity, and dedication to her community are inspiring. She hopes sharing her story and advocating for better coverage will help others living with T1D.
Breakthrough T1D donor funding has contributed to nearly every major T1D advancement in the last 50-plus years. Generous leadership donors who invest in our $100M Campaign to Accelerate help ensure future T1D discoveries while advancing vital efforts, like Lynn’s, to improve care for all those living with T1D.
There is much uncertainty in the world right now, with changes coming so frequently it can feel hard to stay completely informed.
However, Breakthrough T1D Canada can offer certainty that our Canadian-funded researchers are making incredible progress and breakthroughs in T1D research.
Now, more than ever, research is progressing at incredible speed, we can keep that momentum going here in Canada and continue investing in the scientific discoveries that will bring us closer to cures for T1D.
We know there will be questions about how these changes will affect the T1D community going forward, including concerns about potential disruptions to insulin deliveries, devices and other diabetes supplies. Please be assured that we are working hard to gather information as it becomes available, and that we will continue to be transparent and update the community as we learn more.
It’s been said that any challenge can also be an opportunity, and we are taking that approach at Breakthrough T1D Canada.
We have world-renowned T1D researchers working right here in Canada. Canada is where insulin and stem cells were discovered, and where the Edmonton Protocol was developed. And this is why we believe that a made in Canada cure for T1D can be discovered right here too.
We’re the largest charitable funder of T1D research in Canada, and every year thanks to donors, we’re able to give transformational grant funding to the projects that will deliver high impact rather than dispersing funds in small amounts amongst hundreds of small projects.
And we know none of this can happen without the support of our advocates and volunteers. That is why we advocate with the Canadian T1D community to all levels of government for equitable access to treatments and devices, research funding, health regulatory approvals, and more. During this federal election year, we are doubling down on these efforts, with volunteer advocates nationwide championing our shared mission with their local MPs through in-person meetings, letter-writing and social media campaigns.
Since 2019, our Access for All campaign has been advocating provincial governments for more equitable access to diabetes devices including insulins, insulin pumps and technologies like advanced glucose monitors. .
The results of how we invest donor dollars, and the impact of those investments speak for themselves:
Edmonton Protocol
Dr. James Shapiro (Alberta) led the clinical team who developed the groundbreaking “Edmonton Protocol” for successful islet transplantation, first reported in 2000 and supported by Breakthrough T1D (formerly JDRF). Canada is one of the few countries in the world where clinical islet transplantation is available outside of a research setting.
Disease Modifying Therapies
We invest in research around disease-modifying therapies – therapies that slow or stop the disease, rather than just treating the symptoms.
In the early 2000s, Breakthrough T1D started making substantial investments into beta cell replacement research to help the field develop approaches to replace insulin-producing cells lost in people with T1D.
Dr. Timothy Kieffer (British Columbia) was one of the first researchers in the world to show in 2014 that human stem cells can be differentiated into glucose-responsive insulin-producing cells. The procedure these researchers developed set the stage for clinical trials now in progress.
Advancements in stem cell-based therapies for T1D are continuing here in Canada. Vertex trials have thus far reported reduced insulin requirements in several trial participants, including three who are off insulin entirely, and no safety concerns.
By the Numbers
Breakthrough T1D Canada is committed to driving research excellence forward for everyone, everywhere living with T1D:
70 active research grants in Canada
10 Breakthrough T1D-funded clinical trials active in Canada
The transformational breakthroughs Breakthrough T1D has helped fund—including diagnostics, medications and devices—are now helping people with T1D live longer, healthier lives. In the last 50 years of progress, 25 years have been added to the lifespan of a person receiving the latest care in Canada.
Together with our Canadian T1D community, we will remain strong
Canada continues to play a leading role in changing the landscape of T1D research, globally. We want to continue to shine the spotlight on Canadian-led research and our advocacy work to make sure those living with T1D are not forgotten or left behind.
We are incredibly grateful to our donors who continue to support this critical work in these uncertain times. It is crucial that we remain steadfast in our investment in groundbreaking Canadian T1D research today and ensure the pace of progress isn’t slowed down.
Dr. Mahla Poudineh (University of Waterloo), in collaboration with Dr. Leyla Soleymani (McMaster University), is developing a wearable continuous ketone monitor, which can indicate a life-threatening condition called diabetic ketoacidosis (DKA). This device combines novel biology (ketone measurement) with novel engineering (hydrogel microneedles) to produce a groundbreaking new device – the Wearable Aptalyzer.
Biology: Similar to a continuous glucose monitor (CGM), this device will detect biomarkers from the interstitial fluid under the skin. Dr. Poudineh and her team are calibrating the device to recognize and measure real-time ketone levels, something that can currently only be done using urine testing.
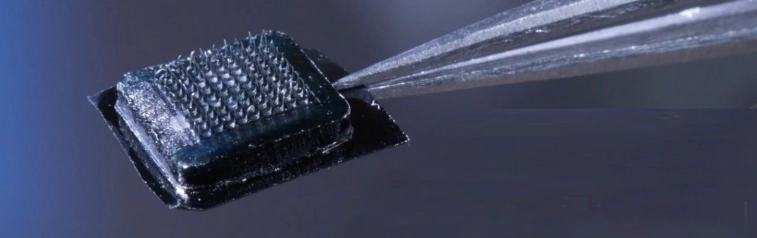
Engineering: Dr. Poudineh’s one-centimeter patch provides a wearable solution that enables real-time continuous biomarker monitoring without the discomfort associated with current canula insertion methods. Her patented patch consists of 100 hydrogel “soft microneedles” placed on the skin like a bandage. The microneedles push into the skin just a few millimeters which allows them to touch interstitial fluid and swell to increase surface area.
Together, Dr. Poudineh and Dr. Soleymani have created a company – Aptec – to commercialize this technology and bring it to those living with T1D.
Dr. Poudineh’s microneedle patch
New Grant: We are excited to announce a second Breakthrough T1D grant for this dynamic team that will expand their work to develop a continuous insulin monitor via the same methods. This would allow people with T1D to have real-time measures of insulin in their system, often known as “insulin on board”, and better adjust against upcoming meals or activities.
Breakthrough T1D Canada congratulates Drs. Poudineh and Soleymani on their recent achievements.
Dr. Mahla Poudineh is making big waves in the medical devices field and was recently named a Tier 2 Canada Research Chair in Health Monitoring BioNano Devices.
Dr. Leyla Soleymani holds a Canada Research Chair in Miniaturized Biomedical Devices and was recently awarded the prestigious Dorothy Killam Fellowship.
Their work will help significantly improve daily living with T1D, while we work towards cures.
A large area of cure-based T1D research is investigating stem cell-based therapy. The goal of this approach is to use stem cells as a renewable source of insulin-producing cells which, when transplanted, would replace beta cells that are destroyed in a person with T1D, thereby allowing them to produce insulin again. This would lessen or eliminate the amount of external insulin required by someone living with T1D (either by injection, pen, or pump) for months or even decades.
Vertex had two active clinical trials for type 1 diabetes cell therapy: VX-880 (FORWARD) and VX-264 (UPWARD). On Friday, Vertex published a press release with updates on its type 1 diabetes (T1D) products.
After review, Vertex will not be moving forward with the clinical development program for VX-264. VX-264 was Vertex’s encapsulated islet cell therapy that does not require immunosuppressive drugs. And while it was generally safe and well-tolerated in clinical trials, it did not meet the efficacy endpoint as measured by C-peptide, a biomarker for insulin levels. What this means is that implanted cells were not producing enough insulin to warrant moving forward with further trials. Currently, C-peptide is our best measurement for determining if insulin is being produced in humans.
In VX-264, the insulin-producing cells were placed in a protective device and then implanted into the body. Analysis of the encapsulation devices is ongoing and may inform future strategies and approaches.
The VX-880 product has been renamed to zimislecel. This trial is continuing as planned, and regulatory submission is expected in 2026. The Phase 1/2/3 pivotal trial for zimislecel is continuing and on schedule for enrollment and dosing. Zimislecel is Vertex’s cell therapy for individuals with severe hypoglycemic (low blood glucose) events. It requires the use of immunosuppressives.
Results from the ongoing trial with VX-880 have demonstrated promising efficacy and safety in all people who received the treatment. Vertex has been working closely with regulators around the world to prepare for submission and is expanding its manufacturing and commercial capabilities to ensure they are prepared for the launch of the drug.
Vertex remains committed to pursuing therapies that could provide “transformational benefits” to the T1D community and is looking at other ways to keep cells safe without the use of standard immunosuppression. These include alternative immunosuppressive regimens, gene-edited hypo-immune manufactured islet cell therapies, and novel devices to encapsulate islet cells.
There is still currently no manufactured cell therapy that is approved for people with T1D. But it is very encouraging that Vertex is preparing to submit for regulatory approval next calendar year and getting ready for the commercial launch.
Developing cell therapies that restore insulin production without the use of standard immune suppression is the focus of Breakthrough T1D’s cell therapies portfolio and is a key focus of our funding strategy.
The discontinuation of VX-264 emphasizes the importance of Breakthrough T1D’s global approach to pursuing multiple strategies to keep cells safe without traditional immune suppression, including those that Vertex is employing.
What does this mean for Canadians with T1D?
For cell therapy to be broadly accessible to people with T1D, the cell product needs to both work and function without or with minimal immunosuppressive therapies. Part of the research process is pivoting and adjusting based on results and moving in new directions to achieve the end goal – in this case – cell therapies that are safe, well-tolerated and ideally don’t require immune suppression.
Breakthrough T1D Canada will continue to monitor results and provide updates as they are made public.
On March 27, 2025 Diabetes Canada released updated Clinical Practice Guidelines for the glycemic management across the lifespan for people with type 1 diabetes.
What are clinical practice guidelines and what do they mean for people with type 1 diabetes (T1D)?
Clinical guidelines are the guiding principles for health care practitioners to stay up to date on best practices in the management and care of people living with all diseases, including type 1 diabetes. As research advances, both in the medication and device landscape, clinicians and experts in the diabetes field meet to discuss the best available evidence and to craft or update the guidelines so that care is optimized.
Knowing your diabetes goals in the context of your life and your circumstances is the first step in deciding upon treatment options with your care team. As you manage your T1D, or the T1D of your family member, it is important to remember that your glycemic targets should be designed to fit into your life, and that conversations with your healthcare provider will help you understand the risks, benefits and considerations of all available treatment options.
This month’s updated guidelines, the first comprehensive update since 2018, are noteworthy because not only do they focus on managing one’s glucose levels across the lifespan, recognizing that children, teens and adults can all have T1D, they also include two exciting and important updates.
What are the new updates and what is their impact on Canadians living with T1D?
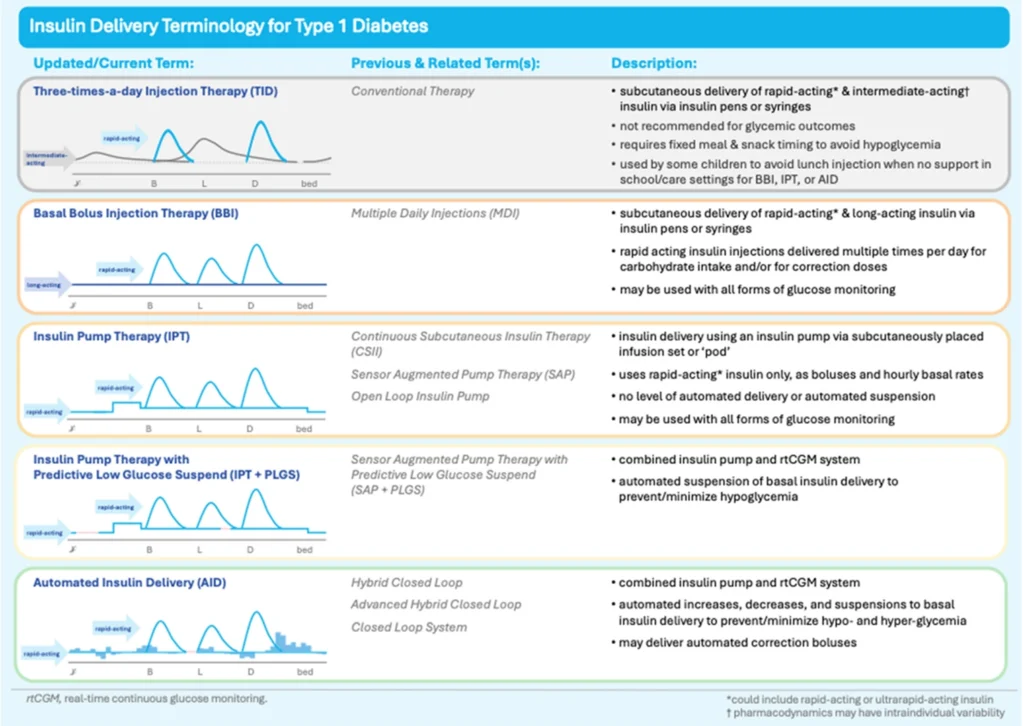
An AID system is a device that automatically adjusts insulin delivery based on blood glucose levels, measured from an accompanying paired glucose monitoring device. It’s also been called an artificial pancreas or hybrid closed-loop system, but AID is the preferred clinical terminology,
The updated guidelines now recommend that insulin be delivered ideally by an insulin pump integrated with a continuous glucose monitor (CGM) (AID) and that these devices be offered to all individuals with T1D, provided they are willing to wear the device and operate it:
Automated insulin delivery (AID) systems (insulin pump and connected continuous glucose monitor) are the preferred treatment method for all individuals to optimize glycemia and/or person-related outcomes, provided the individual is willing and able to wear and operate the devices.
The paradigm shift here is important, as previously the belief was that only those individuals who have met their glucose targets would benefit from this advanced technology. AID systems are beneficial for diverse individuals, regardless of their baseline, or starting glucose levels, and their age or socio-economic status for example. In other words, we need to change the thinking that implies a person with T1D needs to ‘earn’ an AID through already relatively stable management.
AIDs have been shown to keep glucose levels stable and in better range, while also improving sleep and reducing the burden of daily diabetes management (from reducing the fear of hypoglycemia, diabetes distress and improving overall quality of life).
Adjunct therapies for people with T1D
The second noteworthy recommendation is the first of its kind worldwide – adjunctive therapies may now be considered in adults with T1D, based on shared decision-making with the care provider. There is substantial research that has demonstrated the safety and effectiveness of these non-insulin agents such as metformin, glucagon-like peptide-1 receptor agonists (GLP1-RA) or sodium-glucose cotransporter-2 inhibitors (SGLT2i), or what you may know as Ozempic, Wegovy and other GLP-1 agonists, in type 1 diabetes to lower A1c, body weight and insulin doses, when added to insulin.
It is important to recognize individual autonomy of people living with T1D and although this recommendation is not a strong treatment recommendation, as the authors suggest, it is a conditional recommendation that allows for people with T1D to consider their individual health goals and to advocate for treatments that work best for them:
In adults, adjunctive therapy, such as metformin, glucagon-like peptide-1 receptor agonists (GLP1-RA) or sodium-glucose cotransporter-2 inhibitors (SGLT2i), may be considered in addition to insulin to meet individual treatment goals while employing strategies to support safety, efficacy, and tolerability of these medications.
Breakthrough T1D Canada is pleased to see these updated clinical guidelines that will empower people living with T1D to have important conversations with their healthcare provider(s) to discuss the best options for their care. We will continue to advocate for coverage of these therapies and devices so that everyone has access to the treatments and devices that meet their individual health needs.
Patient choice is paramount for diabetes devices, treatments, insulins and insulin administration, as such, Breakthrough T1D will continue to advocate and work with the T1D community to ensure better access, affordability and choice for all Canadians living with T1D.
If you would like to learn more about the updated guidelines, automated insulin delivery devices or adjunctive therapies, please speak to your diabetes health care provider.
Canada’s federal election is underway, and Breakthrough T1D Canada is calling on our T1D advocates across the country to come together and make sure that research and device coverage is part of the discussion.
There are an estimated 300,000 people living with type 1 diabetes (T1D) in Canada and diagnoses are growing more rapidly than general population growth. Over 70% of new T1D diagnoses are in adults and over 80% of Canadians living with T1D are aged 18+
But research works: in the last 50 years of progress, 25 years have been added to the lifespan of a person with T1D receiving the latest care in Canada. Canada has been a world leader in T1D research from the discovery of insulin and stem cells to the creation of the Edmonton Protocol (method of implanting pancreatic islets to treat T1D). Breakthrough T1D has played a pivotal role in nearly every major T1D breakthrough in history—from how HbA1c (a blood glucose measurement) came to be more than 40 years ago to recent advancements like artificial pancreas/hybrid closed-loop systems.
We currently help to fund 65 active research grants in Canada with a total grant value of $63.9M – we invest in the most promising research (e.g. research into new treatments that can halt autoimmunity, stem cell-based therapies that can restore insulin production and more precise diabetes technologies for improved self-management.
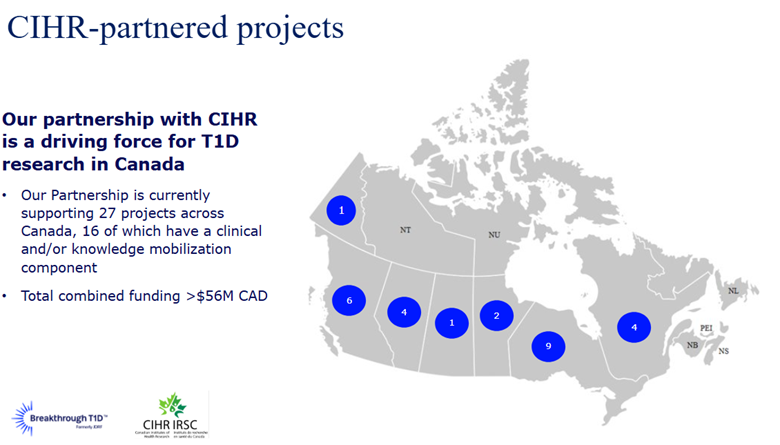
And our advocacy efforts have resulted in improved device access in all provinces and both territories, automatic qualification for the disability tax credit and $30M of government funding directed at T1D research through the Breakthrough T1D Canada -CIHR Partnership to Defeat Diabetes.
Great progress has been made, but we won’t stop until we achieve our ultimate goal, cures for T1D and a world free from this disease.
That is why we need your help to put issues concerning the T1D community at the forefront of this election. Consider meeting with your local candidates, sharing with your T1D journey, and advocating for federal support towards critical T1D research.
To assist volunteers in meeting with local candidates, Breakthrough T1D Canada will be hosting a webinar in both official languages to share best practices and how to make the most successful impact with candidates. This includes information on where to find candidates, how to connect with them, what message we are delivering, and what candidates can do to show their support for Canada’s T1D community.
Additionally, we have developed a simple online form to help people write a letter to candidates and advocate for increased federal support for the T1D community. By filling out this form, a personalized letter will be sent and addressed to the local candidates for Member of Parliament in each riding, highlighting the need to prioritize T1D research and request that they stand with the T1D community. We invite anyone impacted by T1D to participate and share with friends and family to further amplify this message.
Together, we can raise awareness of the issues faced by people living with T1D in this country and ensure it remains top of mind for those who will represent us after the election.
If you have any questions or require any assistance, please reach out to Joey Wong at jwong@breakthroughT1D.ca.
International Women’s Day (IWD) asks us to imagine a gender equal world. A world free of bias, stereotypes, and discrimination. A world that’s diverse, equitable, and inclusive. A world where difference is valued and celebrated. Together we can forge women’s equality. The theme for #IWD2025 is that we can all #AccelerateAction.
International Women’s Day (IWD) has been around for over a hundred years, and many of the issues it addresses unfortunately still remain. IWD reminds us to celebrate women’s achievement, raise awareness about discrimination and to take action to forge gender parity.
Breakthrough T1D Canada is proud to celebrate the achievements of the Canadian women researchers who have blazed a trail in the field of type 1 diabetes (T1D), and who have helped us in our mission of making everyday life better for people living with the disease as we work towards cures tomorrow.
Learn more about Dr. Priscilla White, an early pioneer in diabetes research and treatment, Dr. Dorothy C. Hodgkin who first discovered the three-dimensional structure of insulin, Dr. Helen M. Free, who along with her husband created Clinistix, allowing people to check their glucose at home, a significant advance in disease management. These women played a critical and essential role in advancing understanding of T1D, so that future generations of researchers could build upon their work.
Today, Breakthrough T1D Canada funding helps support many women T1D researchers who are continuing the legacy of those who came before them. They are now charting their own paths by investigating potential cures, new disease-modifying therapies, precision medicine, new and better refined diabetes devices, researching screening and T1D prevention and improving mental health supports to make life better for people living with T1D.
Meet the women researchers who have been supported by Breakthrough T1D Canada funding over the past year:
Dr. Summer Helmi. Postdoctoral Fellow Optimizing Neonatal Porcine Islet Differentiation Using the PBS Mini Vertical-Wheel ® Bioreactor: Advancing Xenotransplantation for Type 1 Diabetes
This innovative project explores a promising approach to treating type 1 diabetes using neonatal porcine islets (NPIs) as a cell replacement therapy. While NPIs offer advantages over other methods, optimizing their production for clinical use remains a challenge. This work could overcome critical hurdles in NPI production, bringing us closer to a more effective and accessible treatment for type 1 diabetes. The project aims to advance porcine islet differentiation strategies and transform diabetes care worldwide.
Dr. Nayara Rampazzo Morelli, Postdoctoral Fellow Investigating a potential drug target in human beta cells during type 1 diabetes
Type 1 diabetes (T1D) is well known for its autoimmune aspects which leads to loss of most of the beta cells in the body and insulin deficiency. How the process of beta cell loss occurs remains uncertain, but recent work indicates that the accumulation of stressed beta cells can accelerate T1D onset. The aim of this study is to evaluate a particular drug target in stressed human beta cells to determine whether this approach could be used to delay the progression of T1D or improve symptoms in people living with T1D.
Dr. Shreyasi Sarkar, Postdoctoral Fellow Assessing the potential of targeting 14-3-3z to restore functional beta cell mass
Dr. Sarkar’s research focuses on identifying new ways to increase beta cell number (mass) to treat T1D. I study a protein called 14-3-3z, and earlier work from Dr. Lim showed that targeting this protein during early development in mice improved insulin secretion and beta cell mass, making this protein a promising target for diabetes treatment. Dr. Sarkar is now exploring a new approach using Antisense Oligonucleotides (a synthetic strand of nucleotide that can modulate protein expression) to target this protein after birth and explore whether similar improvements can be achieved. This may represent a new approach to treat diabetes.
Dr. Alyssa Weinrauch, Breakthrough T1D Canada Centre of Excellence at UBC Dr. Weinrauch’s work focuses on understanding how lipids affect the development and maturation of stem cell derived beta cells. Stem cell derived beta cells offer unlimited potential for curative therapy of T1D. However, currently they do not mature to the same level as human islets, and we believe that lipids may be involved in getting the immature stem cell derived beta cells to that final maturation stage.
Anne-Sophie Brazeau, McGill University – Integrating an online training platform into type 1 diabetes clinical care to empower self-management
Dr. Brazeau and her team will evaluate the implementation strategies for integrating SUPPORT, an online training platform, as part of clinic care and put in place activities to help make health care practitioners aware of the innovation. The aim will be to increase the use and uptake of the platform as well as shorten the time needed to translate research results into practice, ultimately improving the lives of people with T1D.
Valeria E Rac, University Health Network – Connecting diabetic retinopathy screening programs in Ontario.
Dr. Rac and her team will develop a pathway towards the creation of a provincial diabetic retinopathy screening program that includes a provincial registry. The team will also assess the screening needs of different patient populations living with diabetes across the province and set up knowledge gathering workshops to improve access to diabetic retinopathy screening programs, thereby improving eye health for those individuals living with diabetes.
Liris P Smith, Yukon University – Yukon experiences in management of type 1 diabetes: Patient and provider perspectives
Dr. Smith and her team will explore and describe the experiences of people and caregivers of people with T1D in Yukon, recognizing that the needs of the community are unique and that access to care is often limited in rural settings. The grant will allow the team to also describe the experiences of Yukon primary care providers for people living with T1D, with the ultimate goal to improve access to care and management supports.
Principle investigators on Breakthrough T1D-funded research projects
Dr. Shazhan Ahmed Precise Treatment for Pediatric Diabetes: Providing the right care, for the right patient, at the right time, over time.
Dr. Gillian Booth Evaluating innovative health care solutions to improve outcomes for persons with type 1 diabetes using a novel electronic data repository
Dr. Sonia Butalia Aiming for Something Sweeter: Supporting youth with type 1 diabetes during transition from pediatric to adult diabetes care
Dr. Yi-Chen Chun Translational and post-translational regulation of islet prohormones in T1D
Dr. Deborah Da Costa Adaptation and pilot evaluation of a digital intervention targeting the psychosocial needs of individuals with pregestational diabetes: A mixed-methods multi-phase study
Dr. Jayne Danska Microbiome regulation of beta-cell autoimmunity and type 1 diabetes
Dr. Megan Levings Two studies: Harmonizing biomarkers in clinical trials of ustekinumab
Innate & adaptive immune regulation in type 1 diabetes
Dr. Caitlyn Maikawa Polymer materials for glucose-responsive delivery of amylin analogues
Dr. Despoina Manousaki Development of a trans-ancestral genetic risk score for type 1 diabetes
Dr. Shweta Mital Economics of screening and prevention of type 1 diabetes in Canada
Dr. Cristina M. Nostro Three studies: Macrophage-mediated strategies for promoting vascularization and immunotolerance in islet cell replacement therapies
Immune evasive islet-like cells by reduced immune recognition and local immune control
Using novel transplantation strategies and HLA-edited hypoimmunogenic hPSCs to develop a superior islet-like product for T1D treatment
Dr. Sara Nunes de Vasconcelos Development of a new cell-based vascularization approach to improve b-cell survival
Dr. Amanda Oakie Elucidating the role of Notch signaling in the proliferation of human stem cell-derived pancreatic endocrine cell development
Dr. Mahla Poudineh A pH responsive hydrogel microneedle patch for continuous measurement of ketone bodies and glucose
Dr. Kacey Prentice Elucidating the role of the Fabkin hormone complex in metabolic disease
Dr. Elizabeth Rideout Leveraging biological sex and genetics for beta cell-directed precision medicine in type 1 diabetes
Dr. Marie Eve Robinson Teaching adolescents with type 1 diabetes self-compassion (TADS) to reduce diabetes distress: A randomized controlled trial
Dr. Hyekyoung Sung Enabling precision medicine in type 1 diabetes (T1D): leveraging integrative multiomics to understand T1D endotypes for therapy
Dr. Tricia Tang Four studies: Implementing a virtual care platform to improve mental health for type 1 diabetes in rural and remote regions of Interior British Columbia
Using a virtual care platform to deliver peer-led mental health support to rural and remote communities in BC: A randomized wait-list controlled trial of the REACHOUT intervention
Using a virtual care platform to deliver peer-led mental health support to rural and remote communities in BC: A randomized wait-list controlled trial of the REACHOUT intervention
The Mental Health and Diabetes Training Program: Preparing a new generation of providers
Dr. Alanna Weisman Achieving equitable uptake and use of diabetes technologies among adults with type 1 diabetes
Dr. Diane Wherrett Canadian population screening for risk of type 1 diabetes research consortium (CANScreen)
Dr. Holly Witteman Find Your CommuniT1D: Customized virtual peer support for people living with type 1 diabetes
Dr. Xiao Yu (Shirley) Wu Development of targeted nanoparticles for delivering therapeutics to islet cells for treatment of T1D
Breakthrough T1D Canada – an all-women research department. Chief Scientific Officer Dr. Sarah Linklater, along with her team Dr. Lara Green, Dr. Anne Marie MacDonald and Tafadzwa Kadye use their science backgrounds and passion for research to help Breakthrough T1D select and accelerate the most promising T1D research in Canada, and to effectively communicate this research to our stakeholders, government officials and collaboration partners in industry, academia and other non-profit organizations.
Christine Touringy, with support from Dr. Linklateroversees Breakthrough T1D Canada’s Mental Health + Diabetes Strategy as a maternity leave replacement for Amanda Hailman and is helping to maintain the momentum of this program, which works to address the critical gap in healthcare and community programming for mental health supports specific to diabetes.
Breakthrough T1D Canada – A woman led organization In late 2023 Jessica Diniz took on the role of President and CEO of Breakthrough T1D Canada. In April 2023 Helena Gottschling was announced as Board Chair. Both work to ensure Breakthrough T1D Canada can deliver on its strategy, mission, and promise as an organization to donors, supporters, staff and all Canadians affected by T1D.
Breakthrough T1D Canada is proud to continue having both senior leadership and management teams that more than achieve gender parity, skewing heavily female. While acknowledging there is always more to be done, Breakthrough T1D Canada works daily to advance the IWD theme of #AccelerateAction.
Christine MacGibbon has lived with type 1 diabetes (T1D) for 27 years. She raises awareness of the realities of living with this disease in meaningful and unique ways, leveraging her modelling, storytelling, and competitive dance background. She is a bold ambassador for Breakthrough T1D, courageously sharing her story through our Mental Health program and Let’s Talk T1D Education Series on T1D and disordered eating.
The $100M Campaign to Accelerate is Breakthrough T1D’s bold fundraising plan to streamline and speed up the most promising T1D research in Canada and worldwide. Led by passionate philanthropists and dedicated volunteers, this major gift campaign has raised over $86M, funding twice the T1D research than six years ago. Together, we are driving an unstoppable movement to change lives today and accelerate cures tomorrow for people living with T1D like Christine.
Trigger warning: This story references a disordered eating behaviour known as diabulimia (insulin omission to lose weight)
Christine was diagnosed at age nine and remembers having lost a lot of weight and needing to urinate more frequently. She says it got to the point where her teachers were giving her detention because they thought she was trying to get out of class; they didn’t know anyone who had diabetes or its signs and symptoms.
Christine was admitted to the hospital after receiving a T1D diagnosis, which didn’t seem so bad at first; she had a dedicated diabetes care team to help manage her T1D and who helped teach her and her family about the disease. She also met children her age diagnosed around the same time, including one of her best friends to this day. Being surrounded by others who understood what she was going through helped her navigate the first couple of weeks of her diagnosis. Yet once she returned home, she didn’t have the comprehensive diabetes care that she needed to thrive.
Christine had a hard time accepting her new reality of living with a chronic illness. “I didn’t really understand what was happening inside my body and why I needed insulin,” Christine says, “I felt that I was my disease, and it was the reason why I wasn’t able to do so many things.”
Approaching her teenage years, Christine encountered stigma from others regarding her weight, insulin needs, and diabetes technology. This led her to believe that her diabetes was her fault, making her feel undeserving of health or happiness, so she tried to distance herself from her disease entirely. She stopped using her insulin pump, avoided checking her blood glucose levels, and restricted her insulin intake. As a result, she lost weight and received praise for it despite her suffering.
“I struggled with diabulimia for many years,” Christine says, “and at the time, there wasn’t a lot of research surrounding it, so I wasn’t able to get the treatments and support that I needed.”
At age 17, Christine’s HbA1c (the average of her blood glucose levels over 2-3 months) was over 14%. This is much higher than the 7.5% or less recommended for teens with T1D. She was also left without an endocrinologist during the challenging transition period between pediatric and adult care. Throughout her late teens and twenties, Christine was frequently in and out of the hospital and ICU due to diabetes complications that arose from her struggle with diabulimia.
It wasn’t until Christine learned about pathophysiology (the study of how a disease affects a patient) at university that she understood what was happening in her body and realized the damage she was doing to herself by withholding insulin. Talking with others living with T1D and learning about their similar challenges also helped Christine feel less alone in her T1D journey.
Thanks to donor-funded advancements in technology, she is now well enough to pursue a degree in Disability Studies at Toronto Metropolitan University. Christine aims to combat diabetes stigma and spark conversations about how society views and treats diabetes. She advocates for equitable access to T1D support and coverage, ensuring others don’t have to face the same adversities she experienced. She also champions body positivity and mental health in all her work.
Christine is hopeful for the future of T1D research, seeing the advancements in technology, breakthroughs, and new learning in diabetes, which are making lives better now. “When I think of what’s on the horizon and just how much the tech has advanced and how it’s helped me so far, I could see myself living through everything and being OK,”Christine says.
Donors to the The $100M Campaign to Acceleratemake a profound and immediate impact, helping people like Christine, who bravely face the burdens of this relentless disease every day.
To learn more about how you can meaningfully invest through this exciting campaign, please contact:
Do you prefer the sweetness of a Hershey’s kiss, or maybe you like the spice of a cinnamon heart? For most of us, we can grab a handful of Valentine’s Day candy without thinking about it. But for people living with type 1 diabetes (T1D) every snack, every meal, every piece of food eaten must first be calculated for carbs and sugar against the insulin they need to take – just to stay alive.
For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.
Always make sure to check the label carefully, and consider downloading an app, like Roche’s mySugr app, Diabetes M, Quin, which can be connected to a flash glucose sensor (Quin is free but only available on IOS) or apps from your device manufacturers. Visit the website of the manufacturer of your device to find out more.
Carbs and Calslets you take a photo of your meal, and the app searches its library of over 19,000 foods to give you the nutritional information you need.
MyFitnessPal app includes a database of over 14 million foods so you can find out nutritional information about what you’re eating, including the amount of carbs. It has a handy barcode scanner for ready-made products, and you can also add your own foods.
There is a free version and a paid version which has more features. The app is compatible with iOS and Android.
We always want the holidays to be fun for you, or a loved one with T1D, knowing that treats can still safely be enjoyed. It just requires a little extra work and knowing the carb levels of favourite candies.
Remember also to factor in the portion of candy or chocolate you or your child eats to get a more accurate carb count.
Great Value Cinnamon Hearts (25 pieces) contains 15g total carbs, 15g net carbs, 0g fat, 0g protein, and 60 calories.
Hershey Kiss (1 piece) contains 3g total carbs, 2.8g net carbs, 1.5g fat, 0.4g protein, and 27 calories.
Hershey’s Reese’s Peanut Butter Cup (1 package – each 1.5 OZ – 2 cups – 2 1/8″ diameter per cup) contains 23g total carbs, 21.7g net carbs, 12.8g fat, 4.3g protein, and 216 calories.
Jellybeans (10 piece) contains 28g total carbs, 28g net carbs, 0g fat, 0g protein, and 113 calories
Compliments Jujubes (8 candies) contains 33g total carbs, 33g net carbs, 0g fat, 0g protein, and 130 calories.
This May, Matt Varey, a key volunteer with Breakthrough T1D since 2001, will embark on an ambitious two-month long, 7500 km, cycling journey across Canada. As Matt rides Coast-to-Coast for Cures in support of Breakthrough T1D, his goal is that his passion and drive will inspire Canadians to give generously to make each day better for those living with type 1 diabetes (T1D) while driving towards cures.
Matt has held a series of key volunteer roles within Breakthrough T1D. Matt currently serves on both the Breakthrough T1D International Board of Directors as Vice Chair and Breakthrough T1D Canada Board of Directors.
Matt was most recently a senior executive at RBC prior to his retirement in June 2024. Matt joined RBC in 1987 and held a wide range of senior management and executive positions within RBC, including Head of RBC Investments Canadian Financial Planning business. Prior to this responsibility, he was Vice President and General Manager of RBC Suisse, RBC’s Global Private Banking operations in Geneva, Switzerland.
Matt graduated from McMaster University and currently enjoys retirement in Oakville, Ontario, with his wife, Dr. Andrea Jack, or AJ, and their four adult children.
Matt sat down with Breakthrough T1D to share more about his motivations behind taking on such an ambitious fundraiser, and why supporting the T1D community is so important to him.
Breakthrough T1D: Tell us a little bit more about yourself
Matt Varey: I’m 61-years-old, born and raised in Oakville, ON. I had simple, caring parents, both are passed now, an older sister who lives in Calgary, and my brother lives in France. I went to McMaster for kinesiology. I absolutely loved sports, I still do. I was a competitive paddler, played football, rugby, and I biked. My life revolved around sports. But I had another passion, finance and investments. And upon graduation, I came to a fork in the road, did I pursue kinesiology or my other passion. I was always told when you come to a fork in the road, you have to choose one path and follow it through. I got an opportunity to start working at Dominion Securities, so I took the finance fork. I was 23 years old, and I ended up spending 37 years with RBC. I was in leadership for almost my entire career, and it took me so many places – to Saskatoon, Kitchener Waterloo, Toronto, Singapore, Switzerland.
It was also around this time that I met the love of my life, my wife AJ, on a blind date in Muskoka, and we got married about a year and half later. At that point we were living in Toronto, and that started our journey with our family. We have four beautiful adult children. Our oldest works at RBC, our second oldest is a chemical engineer, working to clean water around the world, our third works at Dominion Securities at RBC in the brokerage area, and the youngest works in commercial real estate. AJ is a partner at a dental practice and teaches part-time. And we are both extremely proud grandparents of two grandchildren.
And as I mentioned, my parents are gone, but they were the ones who taught me to always give back. They were very simple and kind people, who were always giving back. I live every day trying to honour what they taught me.
I love the outdoors, lakes, forests, prairies, mountains, anywhere I can just be outside, I love it and feel alive. I love to continue with my middle-aged body in sports, love to be on the bike, love that I’m retired and can follow the markets, I love to read. I am working towards achieving my pilot’s license. So, when I am not on my bike, I like to be in the air. But most of all, I love to be involved with purposeful journeys, and surround myself with kind, caring people dedicated to a purpose.
Breakthrough T1D: You’ve been involved with Breakthrough T1D (formerly JDRF) as a volunteer and board member for over 20 years, how did you first get connected with the organization?
Matt Varey: My relationship with Breakthrough T1D started in 2001, my wife AJ and my four small children were transferred at RBC back from Geneva to Toronto. At that time, we were asked to build a new Canadian business within the bank, and it entailed me and other leaders going across Canada and speaking to employees very passionately and credibly about what they were going to help build. We went coast to coast to Victoria, Newfoundland, Yellowknife. We visited branches, held town halls, we’d do four a day and went onto the next city, to talk about the business.
Banking is a human business based on trust. I had to get out of my introverted shell talking to employees, and so I would ask them – who are you as a person? I want to get to know you as a human beyond just work. I had no idea what Breakthrough T1D (then JDRF) was at the time. And you’d hear from people about their kids, or their sports, and 1 or 2 people, I would ask them about their family, and they would get teary, or speak with a crack in their voice. So, naturally I would probe a bit and ask more, and they would tell me about their family member and their journey with T1D.
So, when I got back from this Canada-wide work trip, I learned about the Breakthrough T1D ‘battle of the banks’ Ride – and thought to myself wow, I have to do this. That spring, I trudged down to City Hall, and was part of the RBC Ride team, I saw so many RBCers enthusiastically giving back, it was so inspiring. I saw all these people raising money for T1D research, and I made this connection to the people who I met along that work trip affected by T1D, and I got the bug. My mother always said, ‘what’s given is yours forever’ and I knew I had a new purposeful journey with Breakthrough T1D.
It all flowed from there. I became the chair of RBC Ride Cabinet, and then the National Cabinet Chair. I saw the power of progress, I saw the dedication, and the passion of people. So I said, I can’t stop at the Ride. And then I met a fabulous mentor, one of the most people important people in my life, Peter Oliver.
Peter was one of founding fundraisers of what was then JDRF, because of his daughter Vanessa, who lives with T1D. He was such a giving person, and he taught me things I will never forget about giving back. He told me: Always think big, never take no for an answer. Do things that will stand out, never underestimate, two is one, one is none, it’s not what’s in front of you, it’s who is on either side of you.
Peter was the definition of a mentor, about what Breakthrough T1D stood for, and the people who worked there. And he knew that he had this young guy named Matt, who would follow anything he asked. I’ve been a Board Member, Vice Chair, Chair of Breakthrough T1D Canada, and I’ve never felt a culture of giving, togetherness and dedication like I did from the people at this organization. This led me to being a board member of Breakthrough T1D International (headquartered in the United States), and now I am currently the Vice-Chair of Breakthrough T1D International.
And this journey can be credited in so many ways to Peter, who was and is, and always will be my north star.
Breakthrough T1D: How did you devise the idea for Coast to Coast for Cures?
Matt Varey: As I retired, in summer 2024 I thought about something my mum always taught me, which was to ‘never stop moving and never let the old man in’. So with mentors like my mum telling me to ‘keep moving’, and Peter Oliver saying, ‘make sure it’s big, make sure it stands out, and make sure it challenges you’, I came up with the idea for the event.
Riding across Canada for 57 days and 7500 kms coast to coast for a cause, it’s doing something different, and honestly – it’s something that scares me, which is good. I also love Canada so much, so that’s part of my journey too. And I knew RBC would always have my back, as a mission, values-based organization, they told me in my retirement if I ever did anything for Breakthrough T1D, they would be involved and support me 100%.
I want to challenge myself, hold true to my mum and Peter. And my wife said she would take two months off work, bring the dog and drive behind me. My wife is my everything and I could never do this without her.
And one evening I made a public proclamation that I was going to do this, and then there was no turning back.
Breakthrough T1D: What are you most excited about for the ride, both personally and for raising awareness of Breakthrough T1D and type 1 diabetes?
Matt Varey: The world is changed by your actions, not by your words. Human beings, deep inside, want to see people accomplish something that is hard, but shows dedication. I think that it attracts human beings to be generous. The sheer wonderment of ‘wow, he did that’. If we’re going to be asking people to help us raise half a million dollars, they want to see your skin in the game.
I’m excited about seeing the generosity of people. I’m an optimist, I always believe tomorrow is going to be better than today. So, I’m excited about people being generous. I’m excited to see Canada for two months with my wife and seeing my former RBC colleagues who I miss dearly.
Breakthrough T1D: Do you have a message for the Breakthrough T1D community?
Matt Varey: We will never ever stop moving forward for cures. Ever. And I am just one of thousands and thousands of incredibly dedicated volunteers who also wake up every day and say the same thing, with even more credibility than myself.
As Mary Tyler Moore, who lived with T1D herself would say, “you can’t be brave, if you’ve only had easy things happen to you.”
And people who live with T1D are brave every day. So please know that my commitment to you is to be brave also. And we will never ever stop until we get to a world free from type 1 diabetes.
To follow Matt’s progress on his journey or to support him, please visit: www.coast2coast4cures.ca
2024 was certainly a year of transformation. We recognized 50 years of grassroots fundraising and advocacy in Canada and in November we became Breakthrough T1D™ Canada. And while we now have a new name and look, our mission remains the same. We are as steadfast as ever about reaching our ultimate goal, a world free from type 1 diabetes (T1D).
Watch: We are Breakthrough T1D
And it is always because of our incredible community of donors, volunteers, and supporters that we never wavered in our mission, seeing progress and breakthroughs across all fields of T1D research. And with successful events and advocacy initiatives across the country, we continued to strengthen our relationship with the amazing T1D community.
From the generosity of our donors, Breakthrough T1D Canada witnessed another transformative year– committing substantive funding to research, developing our partnerships in academia with new fellowships and grants, continuing to support both newly diagnosed families, and our adult T1D community, reinforcing our commitment to being there for anyone living with T1D at any age and any stage of their journey.
And while we work relentlessly towards cures, we continue to try to improve the lives today of the estimated 300,000 Canadians with T1D, through research, advocacy and community engagement.
Highlights from the past year included:
Before transitioning to our new name, we recognized 50 years of JDRF in Canada and shared stories from people who have been living with T1D for over 50 years. Read their stories.
Supporting a novel training award program in Canada that will build capacity for the future of T1D research in Canada through support of racialized women that have been underfunded in academic research.
Globally, together with our affiliates in the United States, United Kingdon, Australia, Netherlands and Israel we are funding more trainees than before.
Convening a successful Kids or A Cure event, bringing youth living with T1D from across the country to meet MPs and Senators in Ottawa to advocate for increased research funding.
Reaching thousands of Canadians affected by T1D through our Breakthrough T1D Education Series, bringing experts into their homes to discuss topics important to them.
Continued support to newly diagnosed families and adults through our Bag of Hope and programs
The Breakthrough T1D-CIHR Partnership to Defeat Diabetes announce 5 new grants in Knowledge Mobilization, to provide researchers and knowledge users the opportunity to work together to use research evidence to improve health services, programs, and policies.
Continued to raise awareness of the importance of clinical trials for moving forward critical T1D research through social media and an Education Series event.
To read more about research updates and stories of people living with T1D, please visit www.breakthrought1d.ca/blog.
As we head into 2025, we pause and reflect on how truly grateful we are for the support of our donors, volunteers and the commitment of the T1D community. Thank you! Together, as we drive toward curing type 1 diabetes, we help to make every day better for the people living with it.



























 For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.
For newly diagnosed families, learning the calculations of carbs against insulin needs can be challenging at first, but with practice and consistency this should become easier over time. And even for people who have been living with T1D for decades, the sugar or carb counts of certain foods can vary, either by brand or a change to the product.  There is a free version and a paid version which has more features. The app is compatible with iOS and Android.
There is a free version and a paid version which has more features. The app is compatible with iOS and Android.